
01
Research Background
Opioids are the most widely used analgesics in the perioperative period.
Research indicates that even patients who have not received opioid treatment are at significant risk for chronic opioid use after major or minor surgeries.
In particular, the dose-dependent induction of hyperalgesia and tolerance by remifentanil may lead to postoperative chronic pain and opioid dependence.
Common adverse reactions include postoperative nausea and vomiting, itching, constipation, excessive sedation, and respiratory depression, with gastrointestinal dysfunction being one of the main factors affecting surgical recovery.
Therefore, it is crucial to minimize opioid use during surgery while providing adequate analgesia.
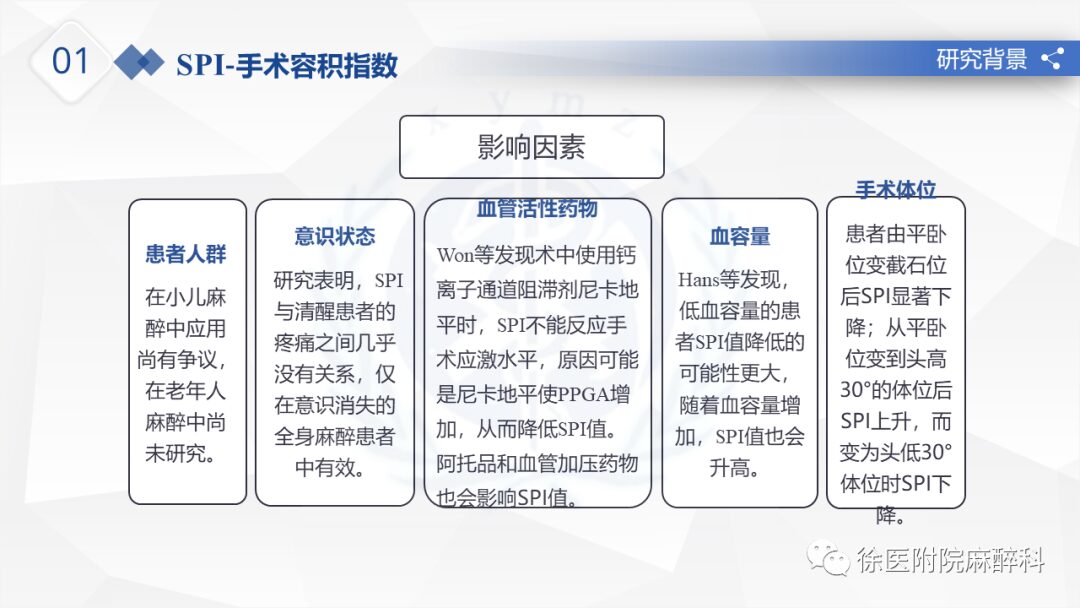
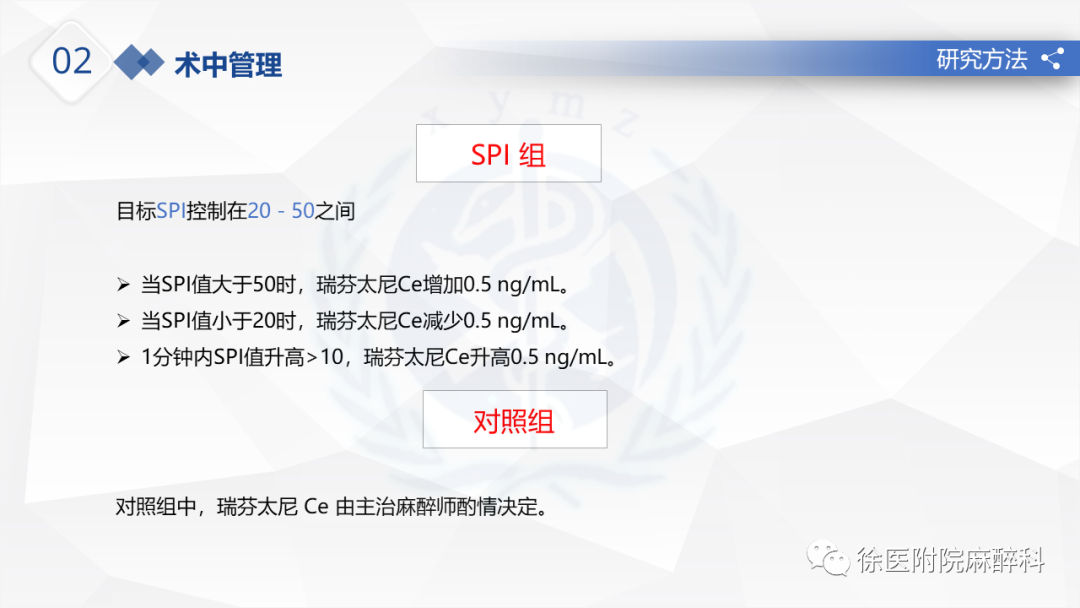
The SPI ranges from 0 to 100, with higher values indicating higher levels of stress and stronger pain stimuli.
Research shows that an SPI value of 20 to 50 reflects adequate analgesic effect.
Changes in SPI greater than 10 or values above 50 indicate insufficient analgesia, while values below 20 indicate excessive analgesia.
02 Pupil Dilation Reflex
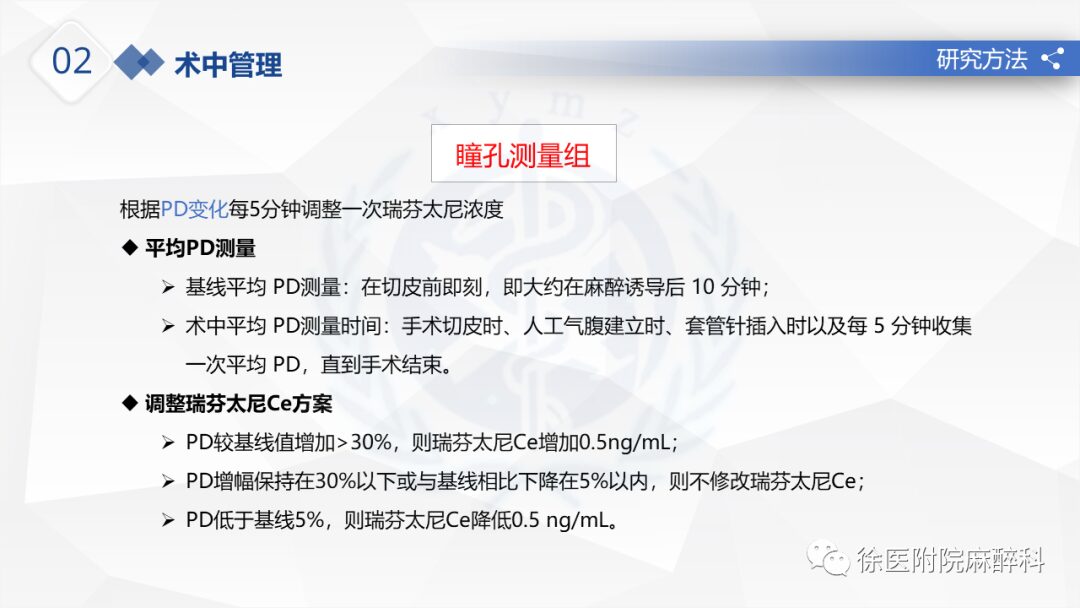
The pupil diameter increases in response to pain stimuli, a phenomenon known as the “Pupillary Dilation Reflex (PDR)”.
In awake subjects, a stimulus such as a loud noise or noxious stimulus activates the sympathetic innervation of the iris dilator muscle, causing the pupil to dilate. However, during general anesthesia, the sympathetic influence on the pupil is abolished, while other parts of the sympathetic nervous system remain functional. Therefore, PDR does not rely on systemic sympathetic activation or peripheral vascular tone.
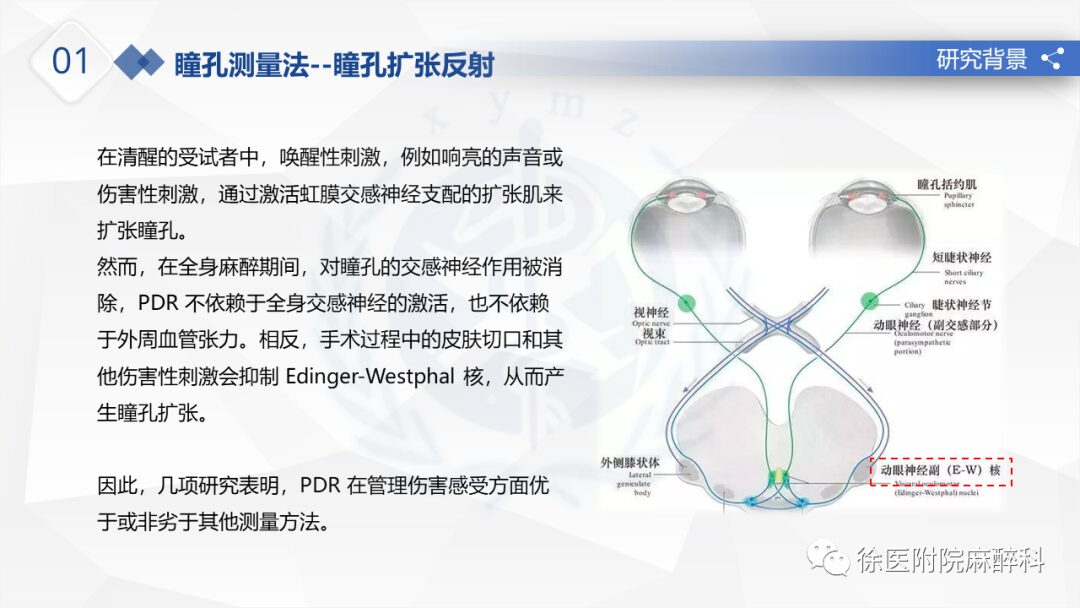
Pupil reflexive dilation can be observed in both awake and anesthetized patients. The degree of pupil dilation is proportional to the intensity of the pain stimulus and inversely proportional to the amount of opioids administered.
Using changes in pupil diameter to guide the control of remifentanil dosage during surgery can relatively accurately control the amount of opioids used.
Research Question:
Can monitoring the pupil during surgery provide more precise control over the use of intraoperative opioids compared to the Surgical Volume Index (SPI)?
02
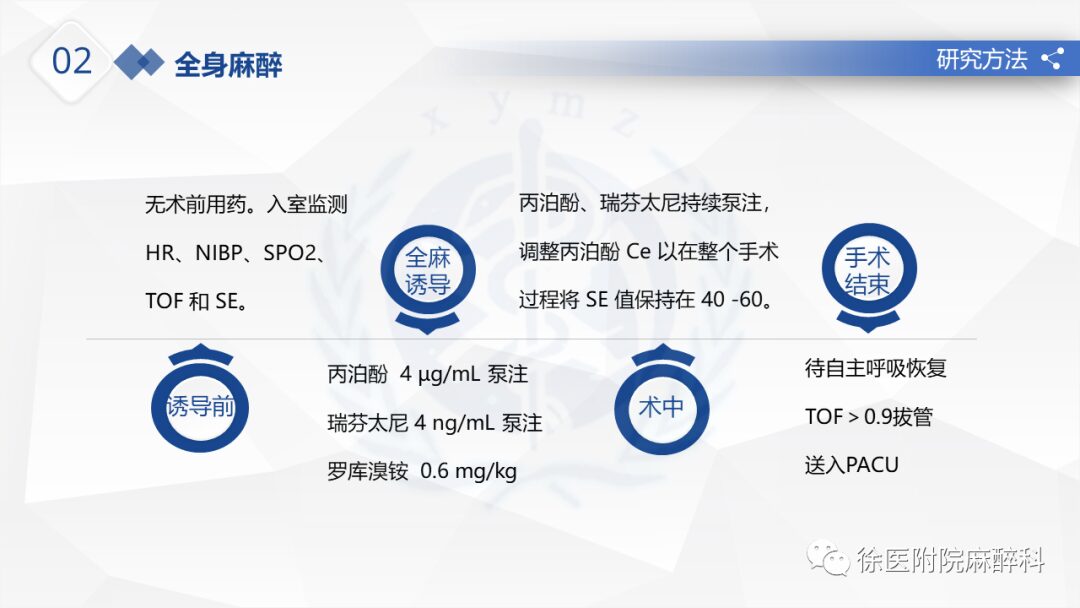
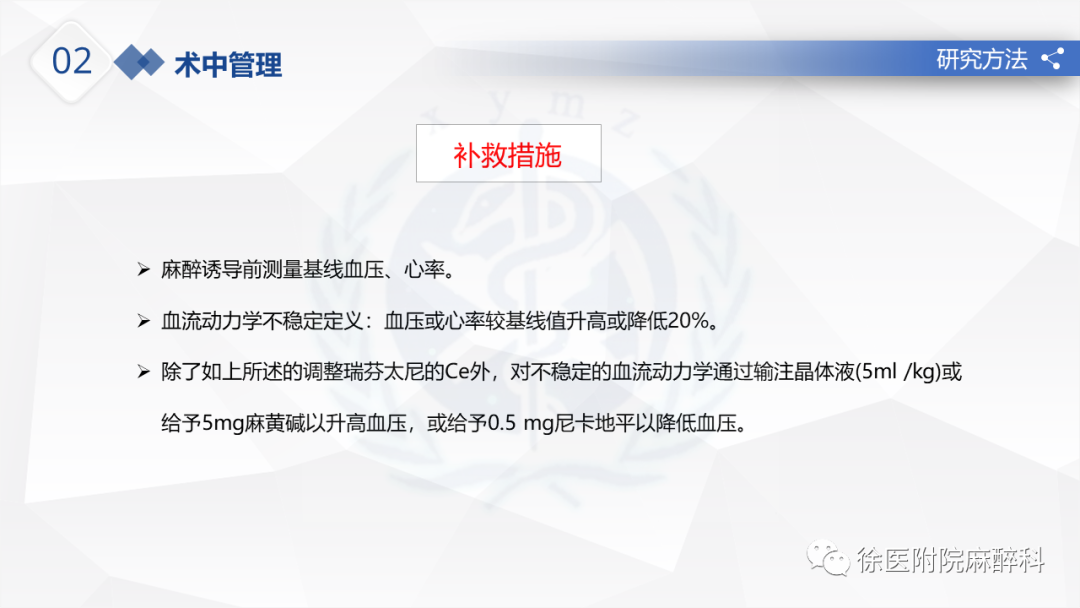
Research Methods
Due to the lack of effective data comparing the efficacy of pupil measurement and SPI monitoring, the trial was conducted in two steps:
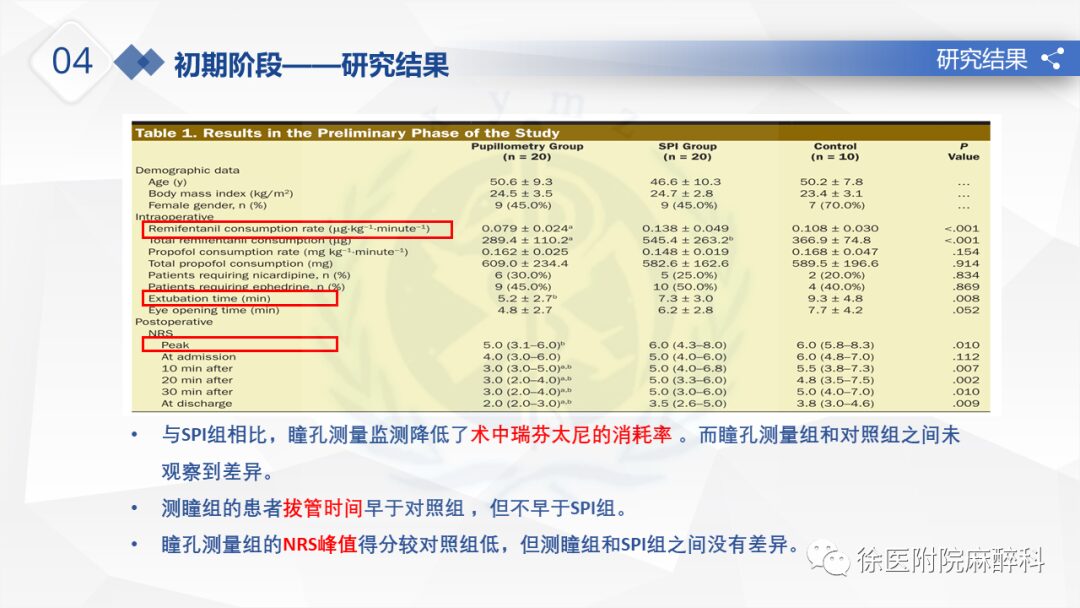
Pilot Phase:
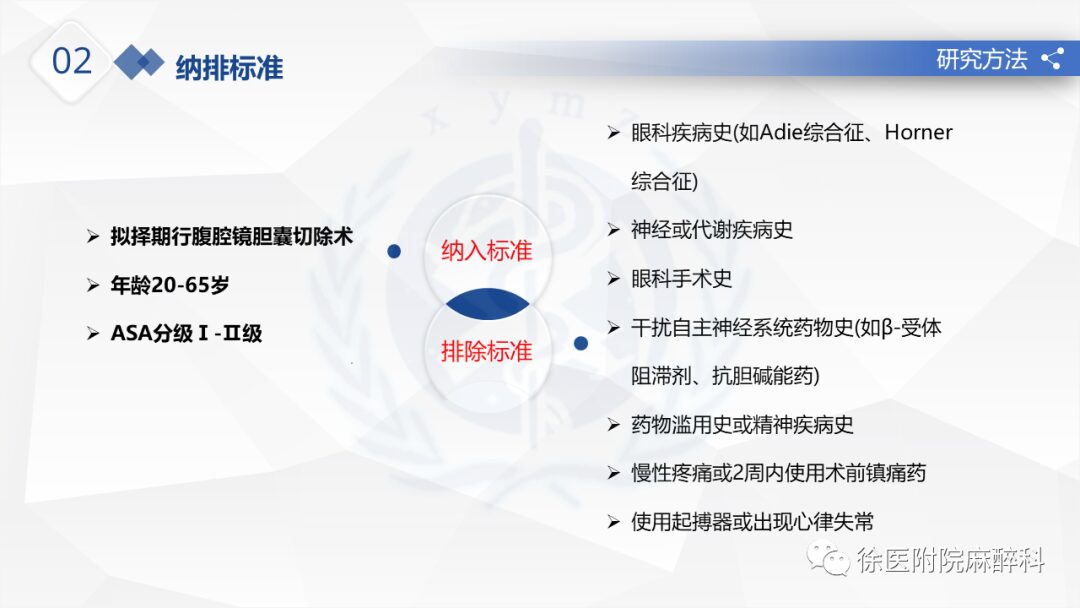
Clinical feasibility assessment of pupil measurement and SPI compared to conventional hemodynamic monitoring (heart rate, blood pressure) was conducted on 50 subjects.
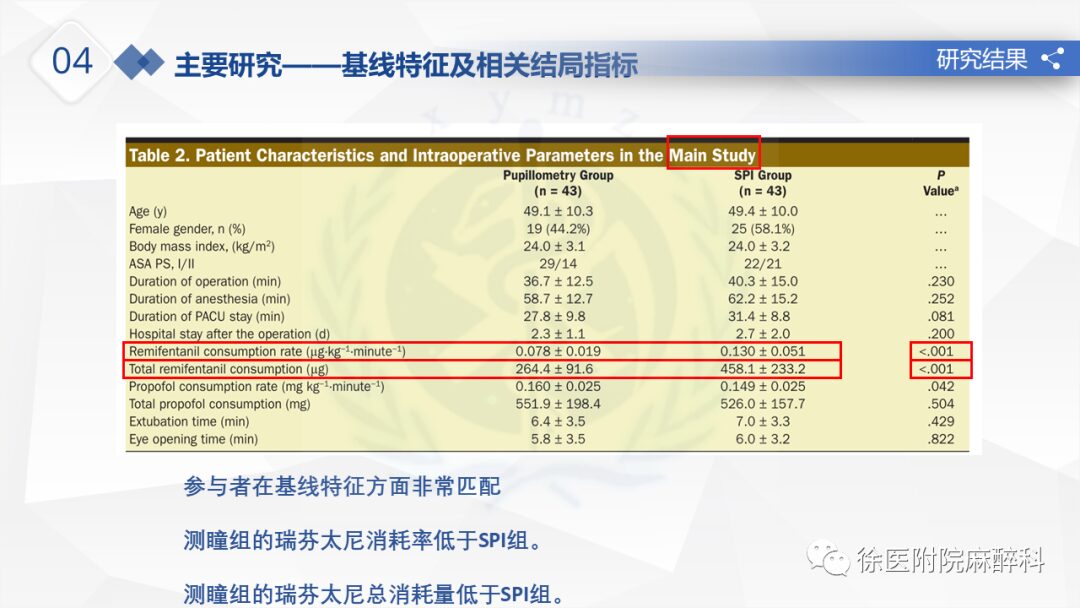
Main Study Phase:
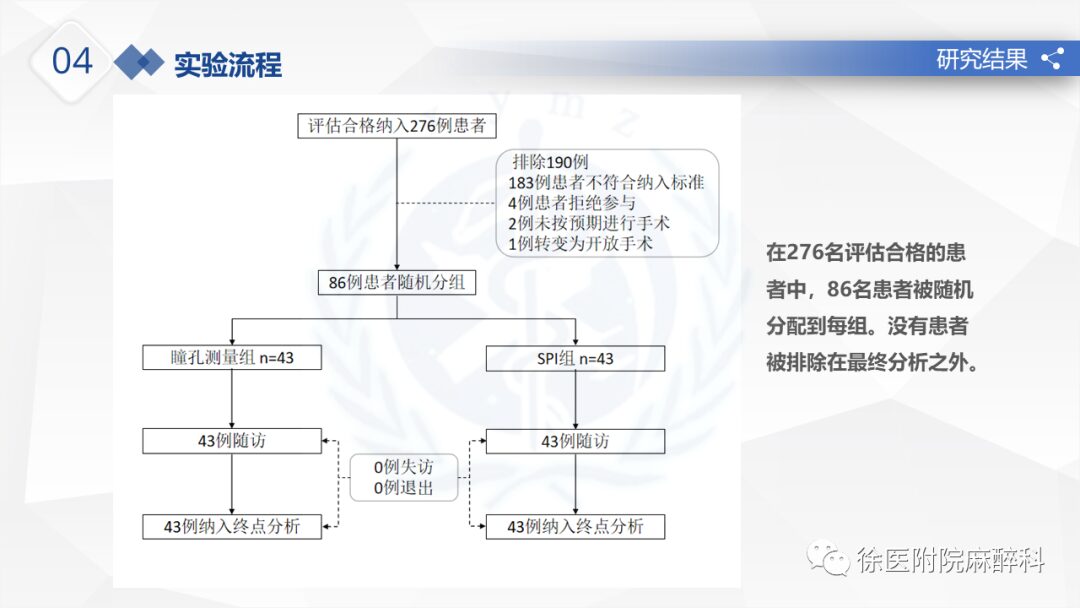
Comparison of the effects of pupil measurement and SPI monitoring in 86 patients from January 2019 to May 2019.
Primary Outcome Measures:
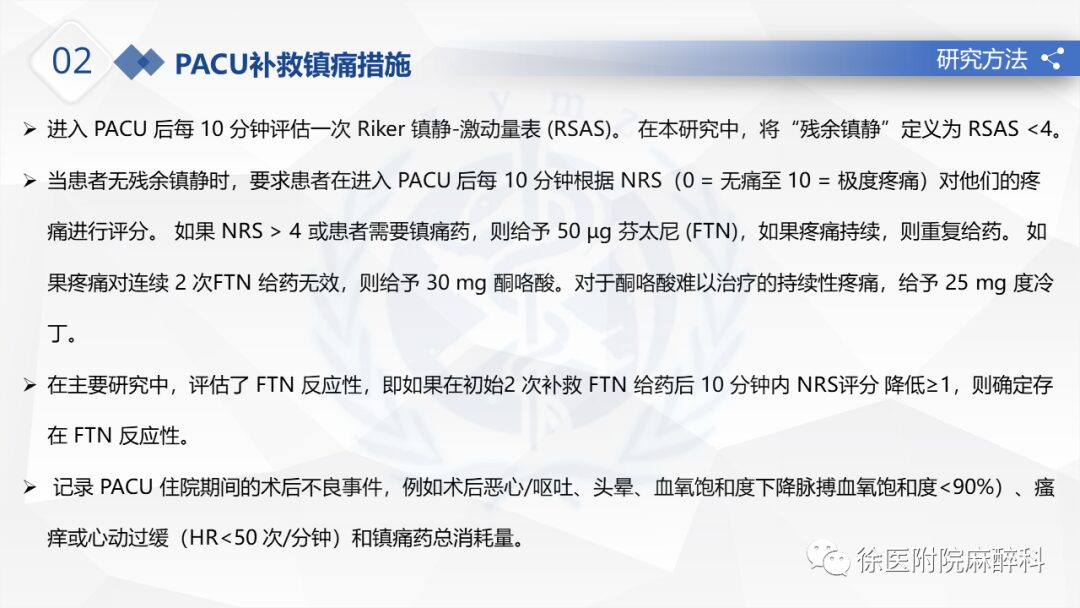
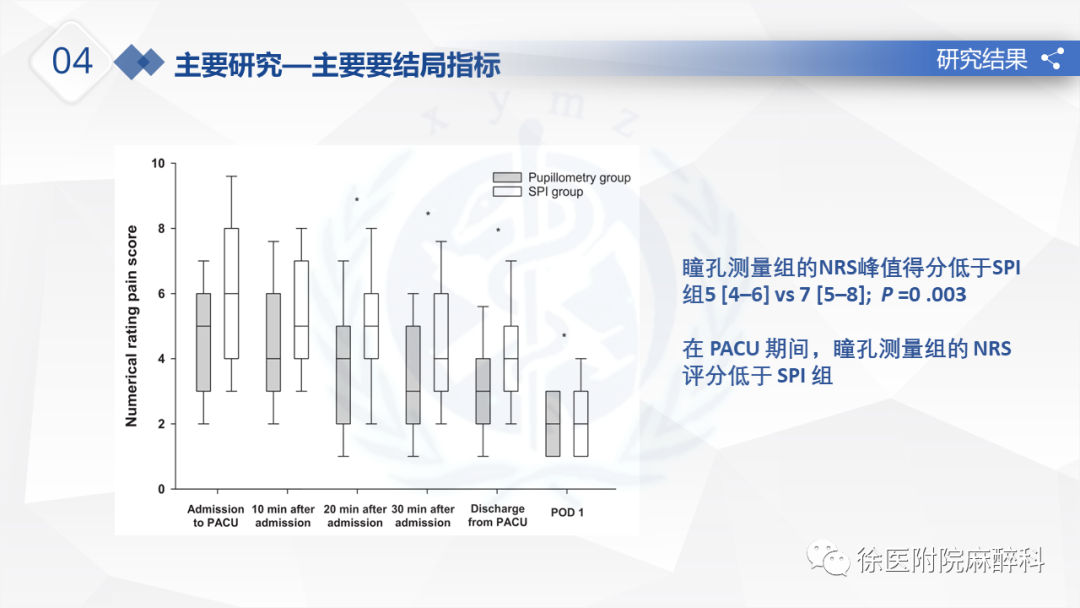
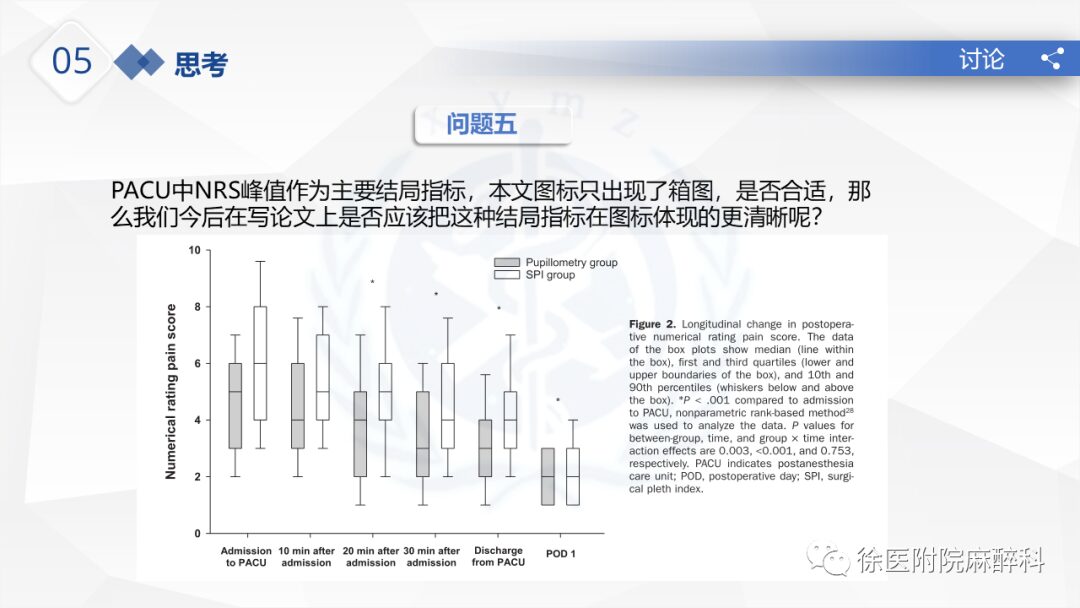
Peak postoperative numeric rating scale (NRS) during PACU
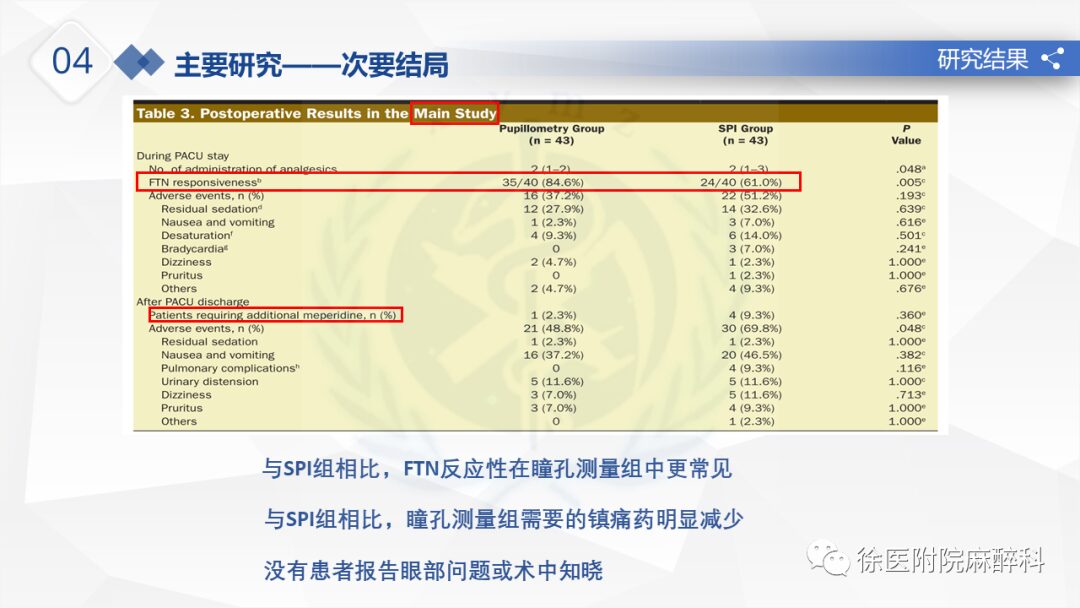
Secondary Outcome Measures:
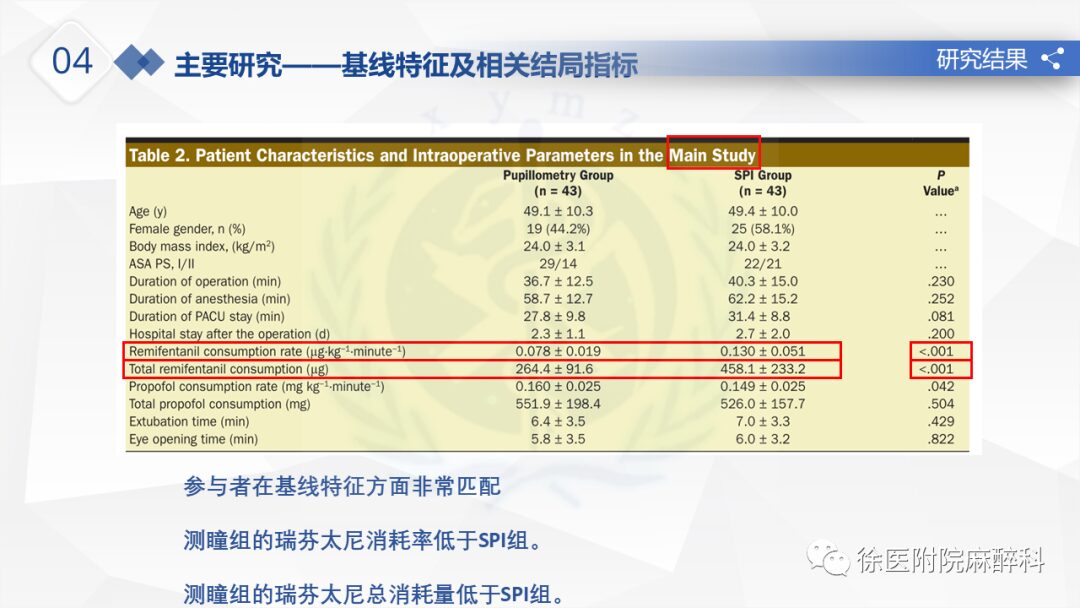
Intraoperative remifentanil consumption rate
Percentage of opioid responses
Number of analgesic uses during PACU stay according to the planned protocol
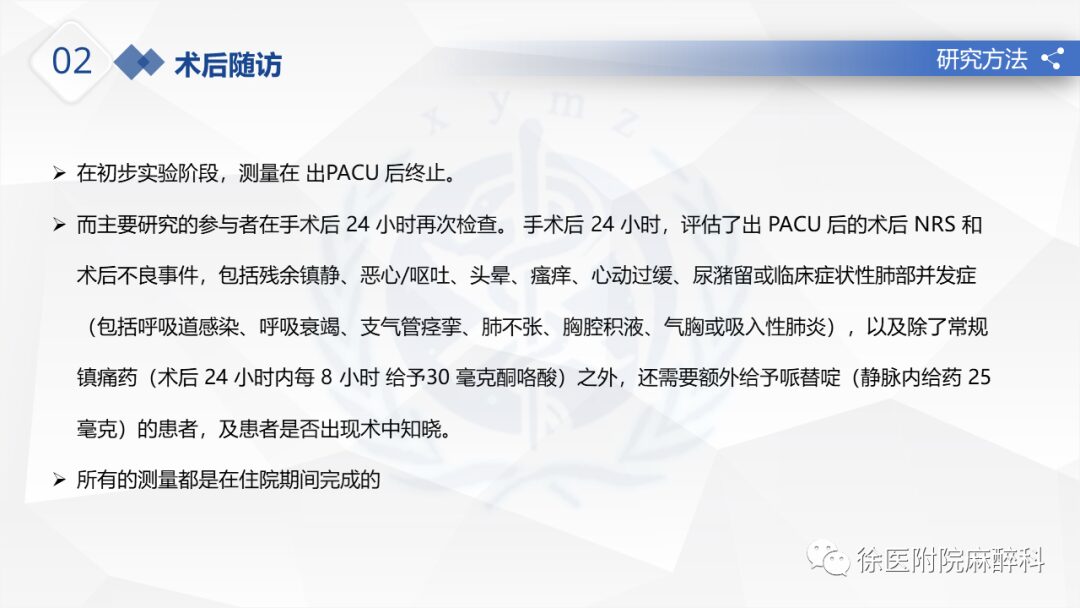
Number of additional pethidine doses given after leaving PACU based on routine analgesia
Postoperative complications related to opioids
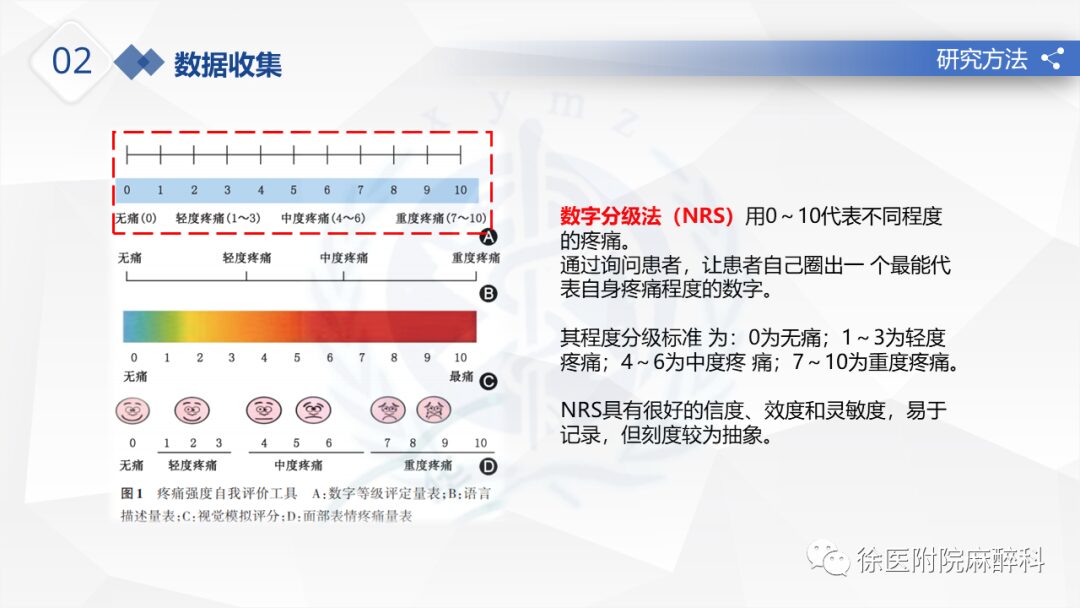
The VAS is the most widely used unidimensional measurement tool. A straight line (generally 10 cm long) is drawn, one end representing no pain and the other end representing extreme pain, allowing the patient to mark a cross at the point that best reflects their pain level. The assessor estimates the patient’s pain level based on the location of the cross on the line.
Although VAS is a simple and effective measurement method, it requires abstract thinking, and necessary sensory, motor, and perceptual abilities are needed when marking the line with a pen, leading to a high failure rate when used with elderly patients. Therefore, VAS is not suitable for individuals with lower educational levels or cognitive impairments. When used with individuals with mild impairments in abstract thinking, a vertical orientation is better than a horizontal one.
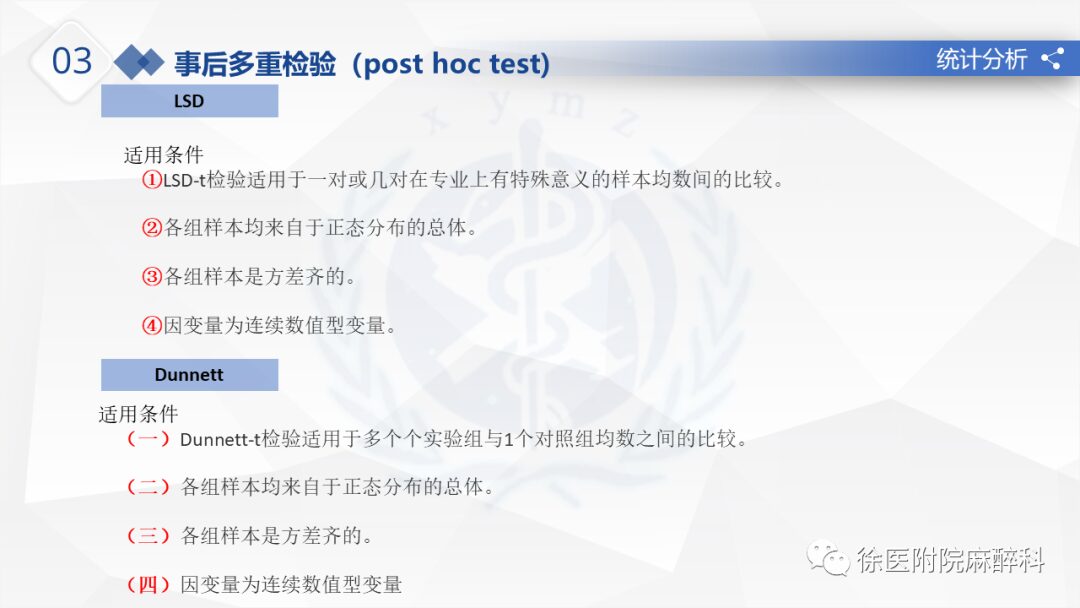
03
Statistical Analysis
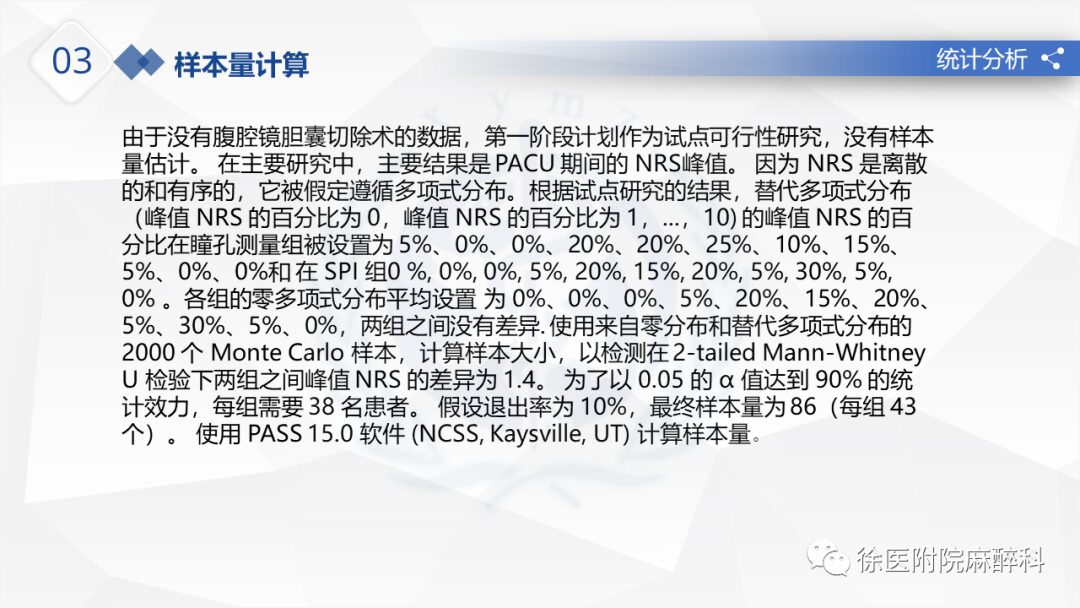
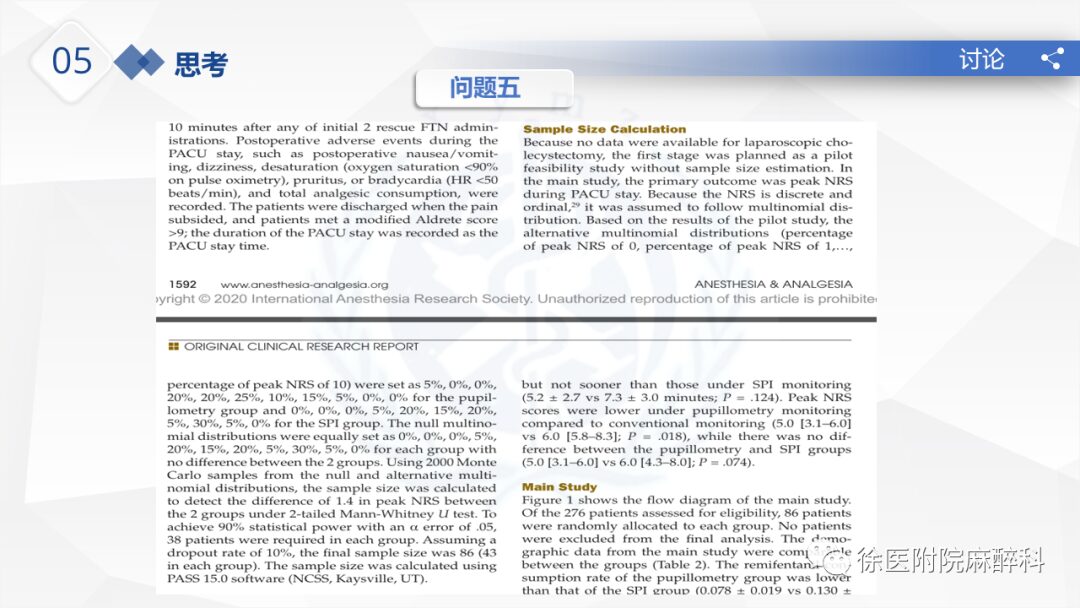
Sample Size Calculation:
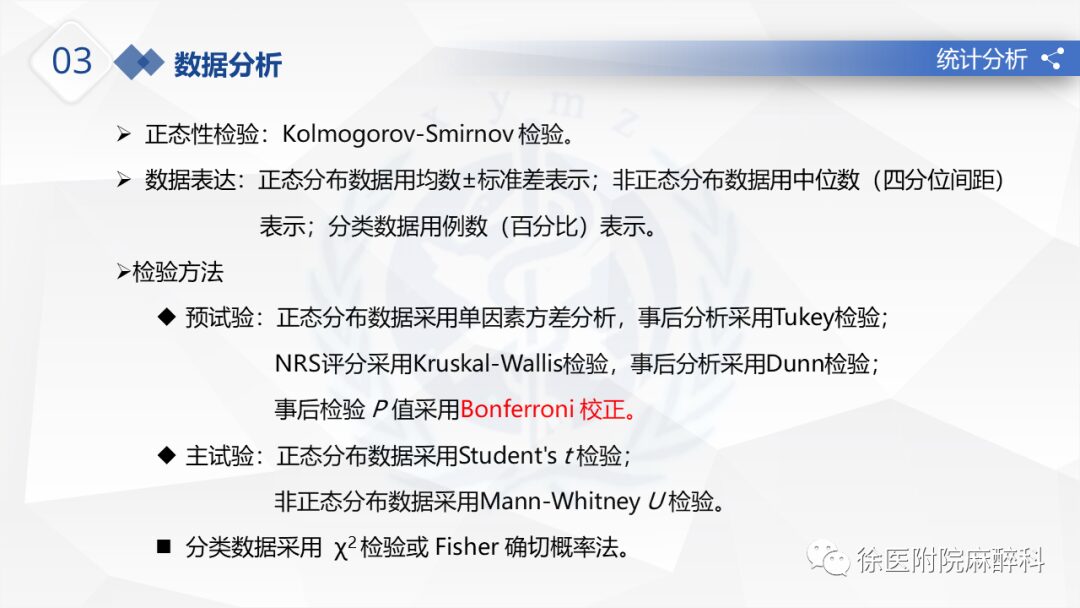
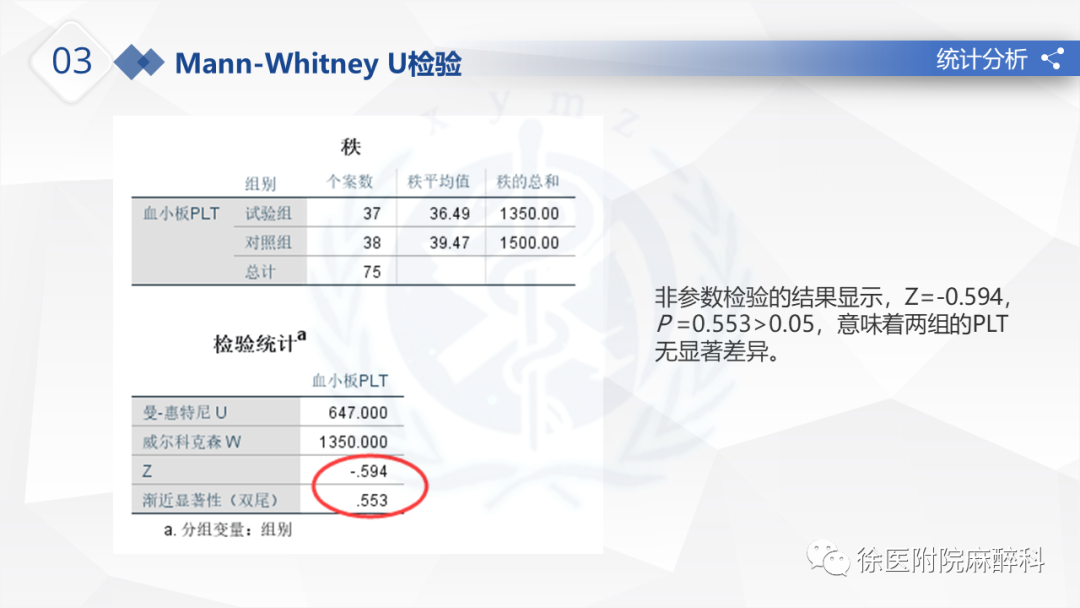
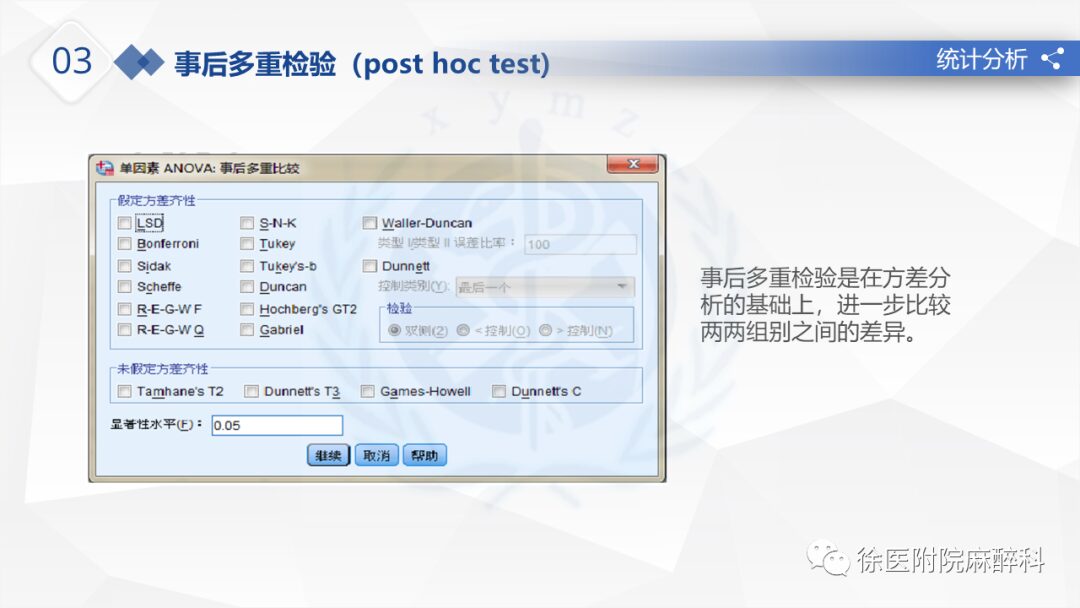
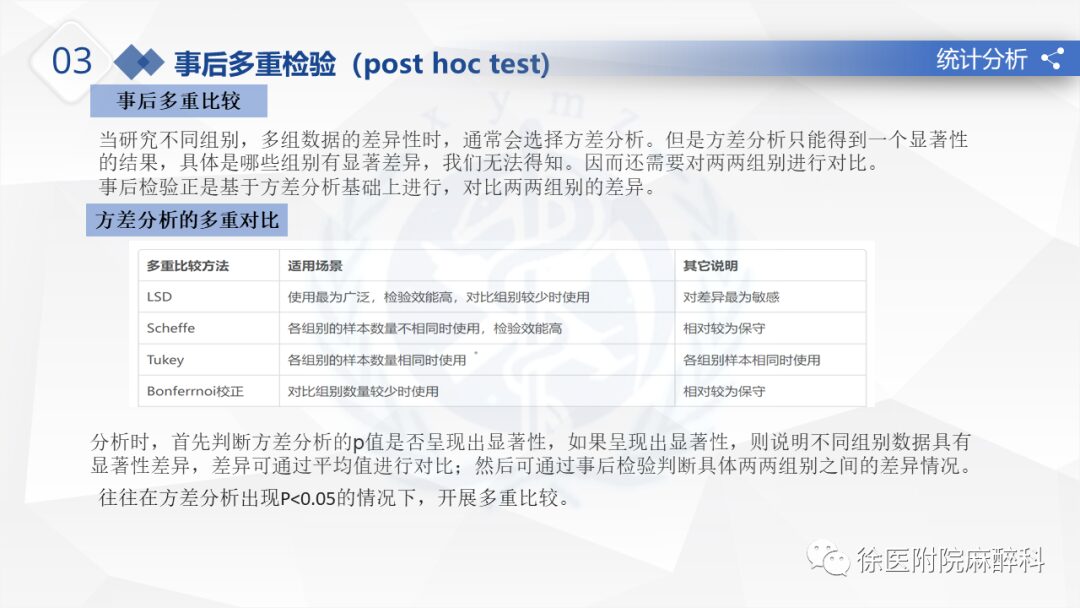
Data Analysis:

04
Research Results
05
Discussion
Advantages:
1. Postoperatively, pupil measurement not only reduced postoperative pain but also improved FTN reactivity by reducing analgesic use.
2. These results may suggest that monitoring pupil dilation can prevent the development of opioid-induced hyperalgesia by reducing remifentanil consumption.
Limitations:
1. High doses of opioids completely inhibit PDR, so pupil measurement monitoring should not be generalized to surgeries requiring high doses of opioids.
2. Postoperative pain can be influenced by many variables beyond opioid use. It cannot be guaranteed that confounding effects are completely excluded.
3. The peak NRS was used as the primary outcome, and the number of analgesic doses as a secondary outcome was assessed without considering the interrelationship between them; using analgesics in high NRS scores affects subsequent NRS scores. Therefore, to confirm the conclusions of this study, future research should employ joint hypothesis testing to analyze the interrelated outcomes (peak NRS and analgesic dosage).
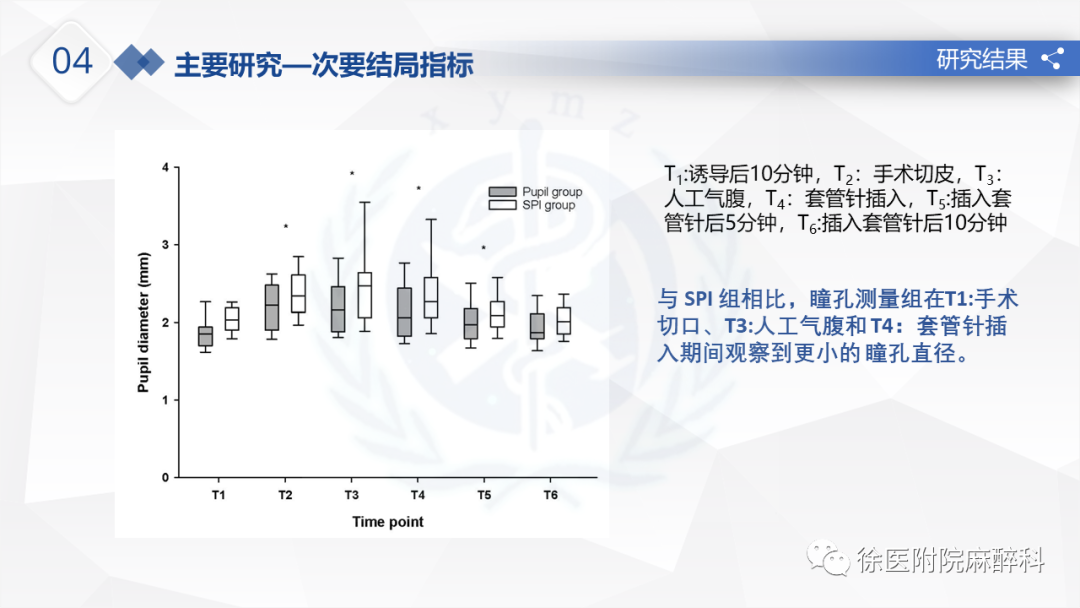
4. SPI was continuously recorded during the experiment while pupil diameter was measured every 5 minutes. During the 5-minute interval, the pupil measurement method could not detect significant changes in the state of nociception. Therefore, pupil diameter should be measured at intervals of <5 minutes when a series of noxious stimuli (surgical incision, inflation, and laparoscopic cannula insertion) are applied.
Conclusion:
1. Intraoperative pupil measurement monitoring reduces remifentanil consumption and postoperative pain.
2. Monitoring the pupil during surgery is a reasonable choice for intraoperative analgesia.

XU Medical University
Reviewed by | Liu Su
Edited by | Zhao Qiu