
Table of Contents
| Q1: How to sample for reverse osmosis water and endotoxin detection in dialysis fluid? |
| Q2: What are the control standards for dialysis fluid? |
| Q3: Does concentrated dialysis fluid also need to be tested for endotoxins? What is the standard? |
| Q4: How to handle excessive bacterial counts in reverse osmosis water for hemodialysis? |
| Q5: What are the differences between hemodialysis and hemofiltration? Why do bedside hemofiltration machines not require dedicated machines for infectious disease patients? |
| Q6: Are the regular dialysis area and isolation dialysis area relative divisions? Or must there be a physical barrier? |
| Q7: Is it necessary to set up a buffer zone between the regular dialysis area and the isolation dialysis area? |
| Q8: Can dry and wet storage rooms be in the same room? |
| Q9: In the absence of a dedicated emergency dialysis machine, should emergency dialysis patients be placed in the regular dialysis area or the isolation dialysis area? |
| Q10: After emergency hemodialysis patients use a dedicated emergency machine and test positive for bloodborne infection markers, how should the hemodialysis machine be disinfected? |
| Q11: Can hemodialysis machines used by patients with bloodborne infectious diseases be disinfected and then used for regular patients? Can nurses in the isolation dialysis area perform procedures for patients in the regular dialysis area? |
| Q12: Can the touch screen of a hemodialysis machine be wiped with chlorine disinfectant? |
| Q13: Can medical waste bins be placed in the dialysis area? |
| Q14: Can curtains be hung in the hemodialysis room? |
| Q15: Do staff need to change shoes when entering the dialysis area? Do other personnel need to wear shoe covers when entering the hemodialysis room? |
| Q16: Should medical waste generated by hemodialysis patients in the isolation dialysis area be collected separately and marked? |
Q1: How to sample for reverse osmosis water and endotoxin detection in dialysis fluid?
According to the original Ministry of Health’s “Standard Operating Procedures for Blood Purification (2010 Edition)”, the sampling site for bacterial and endotoxin detection in reverse osmosis water for hemodialysis is the end of the reverse osmosis water delivery pipeline. This “end of the reverse osmosis water delivery pipeline” should refer to the connection point between the water delivery hose after the hemodialysis machine and the hemodialysis machine. Before sampling, all necessary materials should be prepared, and the water treatment equipment and hemodialysis machine should be operated for at least 10 minutes.
The steps are as follows:① Disconnect the water delivery hose from the connection device of the hemodialysis machine’s internal pipeline.② Use a 75% ethanol swab to disinfect the end of the water delivery pipeline three times.③ Allow reverse osmosis water to flow freely for about 30 seconds.④ Use a sterile, non-pyrogenic sampling bottle to collect 2 ml of reverse osmosis water in the specimen bottle.⑤ Cap the specimen bottle to prevent contamination.Send the specimen to the laboratory for testing as soon as possible.⑥ The entire sampling process should follow the principles of sterile technique to avoid specimen contamination.The endotoxin detection specimen for dialysis fluid should be sampled at the connection point between the dialysis fluid circulation pipeline and the inlet of the dialyzer (lower interface).
The specific steps are as follows:① Use a 75% ethanol swab to disinfect the connection point between the dialysis fluid circulation pipeline and the dialyzer inlet.② Separate the dialysis fluid circulation pipeline from the dialyzer inlet.③ Allow the dialysis fluid to flow freely for about 30 seconds to rinse and clean the sampling port.④ Use a sterile, non-pyrogenic disposable syringe to aspirate 2 ml of dialysis fluid from the lumen of the dialysis fluid circulation pipeline into the specimen bottle.⑤ Cap the specimen bottle to prevent contamination.Send the specimen to the laboratory for testing as soon as possible.⑥ The entire sampling process should follow the principles of sterile technique to avoid specimen contamination.The detection of bacterial concentration in reverse osmosis water and dialysis fluid can refer to the above sampling methods.
Q2: What are the control standards for dialysis fluid?
For the quality standards of endotoxins in dialysis fluid, currently, only the “Standard Operating Procedures for Blood Purification (2010 Edition)” requires that dialysis fluid endotoxins be tested at least once every 3 months, with endotoxins ≤2 EU/ml. There are no other standards or normative documents, so the standard of dialysis fluid endotoxins ≤2 EU/ml should still be implemented. However, there is a question: dialysis fluid is prepared by mixing concentrated dialysis fluid and reverse osmosis water in proportion, with reverse osmosis water having endotoxins ≤0.25 EU/ml and concentrated dialysis fluid having endotoxins ≤0.5 EU/ml. The endotoxin level of the dialysis fluid prepared from reverse osmosis water and concentrated dialysis fluid should not exceed 0.5 EU/ml, while the control standard for dialysis fluid endotoxins in the “Standard Operating Procedures for Blood Purification (2010 Edition)” is ≤2 EU/ml. This may consider the contamination of reverse osmosis water by the main water supply pipeline.
The dialysis fluid directly used for hemodialysis treatment is mixed from reverse osmosis water and concentrated dialysis fluid in a certain proportion. Therefore, the endotoxin levels of reverse osmosis water and concentrated dialysis fluid will definitely affect the endotoxin levels of the dialysis fluid.
Q3: Does concentrated dialysis fluid also need to be tested for endotoxins? What is the standard?
Since concentrated dialysis fluid is a product provided by the manufacturer, hospitals do not need to routinely monitor the quality of concentrated dialysis fluid. When there are suspicions that adverse dialysis events are related to concentrated dialysis fluid, corresponding sampling and monitoring can be conducted. YY 0598–2015 “Concentrates for Hemodialysis and Related Treatments” requires that the endotoxins in hemodialysis concentrated dialysis fluid be ≤0.5 EU/ml.
The dialysis fluid that undergoes dialysis through the hemodialysis machine is prepared from concentrated dialysis fluid and reverse osmosis water in a certain proportion. The quality of concentrated dialysis fluid will inevitably affect the quality of the dialysis fluid directly used for hemodialysis treatment. Therefore, the microbial indicators and endotoxin levels of concentrated dialysis fluid must be controlled within acceptable limits to ensure the quality of dialysis fluid and the safety of hemodialysis patients.
Q4: How to handle excessive bacterial counts in reverse osmosis water for hemodialysis?
According to management requirements, each medical institution should regularly test the bacterial counts of reverse osmosis water for hemodialysis, and timely intervention should be carried out for excessive bacterial counts. For excessive reverse osmosis water, first, eliminate problems in the sampling, storage, transportation, and testing stages to rule out the existence of false positives. Intervention measures include two aspects: first, find the cause of the excess, and second, rectify the identified causes.
According to relevant regulatory requirements, the sampling of reverse osmosis water in hemodialysis rooms of medical institutions generally has three sampling points: ① the outlet of the reverse osmosis machine (Point A). ② the connection point between the water delivery hose behind the hemodialysis machine and the internal pipeline of the dialysis machine (Point B). ③ the end of the main water delivery pipeline (Point C). Different sampling points for excessive bacterial counts in reverse osmosis water have different meanings and causes, thus requiring different intervention measures (Table 5-9).
Excessive reverse osmosis water is usually caused by three main reasons: ① failure of the reverse osmosis machine. ② biofilm formation in the main water supply pipeline. ③ biofilm formation in the water delivery hose of the hemodialysis machine. Based on the three main reasons for excessive reverse osmosis water and the different sampling points for excessive reverse osmosis water, the following inferences can be made.
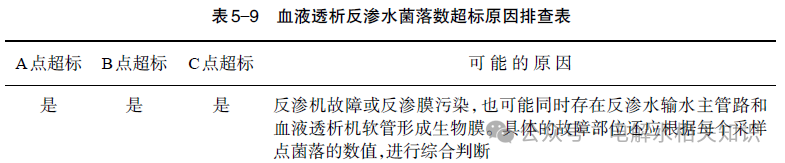
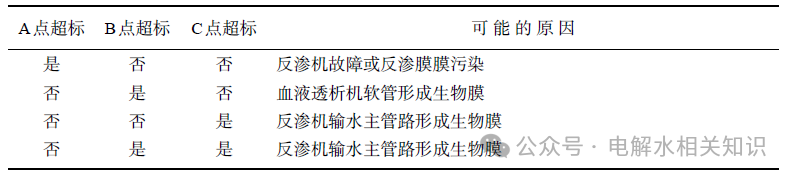
Different causes of excessive bacterial counts in reverse osmosis water for hemodialysis require different intervention measures. If it is due to a malfunction of the reverse osmosis machine, a water machine engineer should be called to repair and maintain the water treatment machine; if it is due to biofilm contamination of the reverse osmosis membrane, disinfection or replacement of the reverse osmosis membrane should be carried out; if it is due to biofilm formation in the main water supply pipeline of the reverse osmosis machine, thorough disinfection of the main water supply pipeline should be performed; if it is due to biofilm formation in the water delivery hose of the hemodialysis machine, disinfection or replacement of the water delivery hose should be carried out.
For disinfection of reverse osmosis membranes, reverse osmosis water supply pipelines, and dialysis machine hoses that have developed biofilms, a compound peracetic acid preparation can be used to thoroughly eliminate biofilms and kill free bacteria in reverse osmosis water. In terms of equipment maintenance and upkeep, adjust the existing cleaning and disinfection procedures and processes of the water treatment equipment, increase the frequency of disinfection, shorten the disinfection cycle, and prevent the reformation of biofilms in the reverse osmosis water system, thus affecting the quality of reverse osmosis water.
Q5: What are the differences between hemodialysis and hemofiltration? Why do bedside hemofiltration machines not require dedicated machines for infectious disease patients?
Hemodialysis and hemofiltration are different methods of blood purification. Besides both aiming to purify blood, there are some differences between the two methods (Table 5-10).
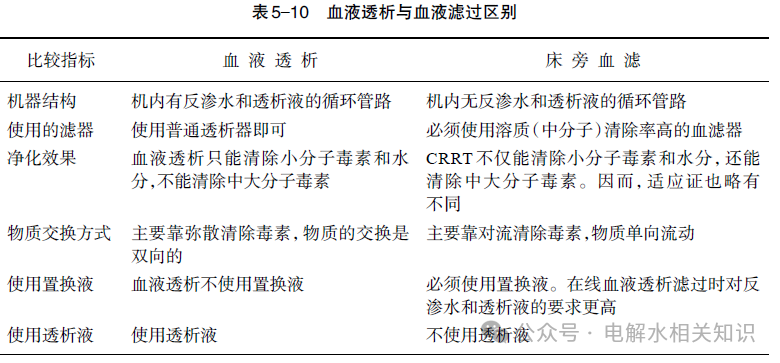
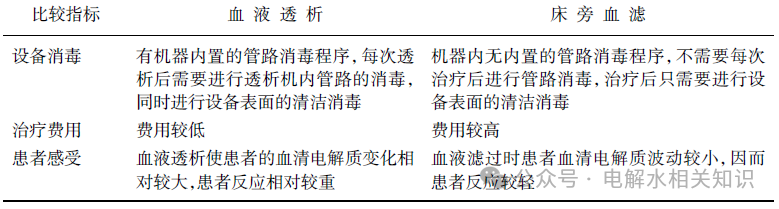
Disinfection of the internal pipeline of the hemodialysis machine after each dialysis session is a preventive measure aimed at avoiding bacterial proliferation within the machine and even biofilm formation. Based on the above differences, bedside hemofiltration machines (CRRT) do not have internal reverse osmosis water and dialysis fluid circulation pipelines, thus eliminating the risk of cross-infection to patients through the internal machine. Therefore, it is unnecessary to equip dedicated bedside hemofiltration machines for infectious disease patients. However, after each treatment, the surface of the hemofiltration machine must be cleaned and disinfected to reduce the risk of cross-infection.
There is also a type of dialysis machine that can perform both hemodialysis and hemofiltration simultaneously; this treatment modality is called hemodialysis with hemofiltration (HDF). Machines with hemodialysis and hemofiltration capabilities do not differ in appearance from regular hemodialysis machines, and many of the internal pipelines are also similar to those of regular hemodialysis machines. Therefore, after each hemodialysis treatment, the procedures for disinfecting internal pipelines and cleaning and disinfecting the surfaces of external items should be managed similarly to regular hemodialysis machines.
Q6: Are the regular dialysis area and isolation dialysis area relative divisions? Or must there be a physical barrier?
For bloodborne diseases such as hepatitis B, hepatitis C, AIDS, and syphilis, the transmission routes are typically through blood and body fluids, with contact transmission also increasingly being emphasized. To effectively block the transmission between infectious disease dialysis patients and non-infectious disease dialysis patients, a physical barrier should be constructed between the isolation dialysis area and the regular dialysis area. This can effectively block contact between infectious disease dialysis patients and non-infectious disease dialysis patients and control the movement of medical personnel between the isolation dialysis area and the non-isolation dialysis area. Since these diseases do not transmit through air or droplets, the physical barrier can be either a full-height partition or a half-height partition, with no clear definition on the height of the barrier. However, for patients with airborne transmitted diseases, dedicated isolation dialysis areas must be separate rooms.
Q7: Is it necessary to set up a buffer zone between the regular dialysis area and the isolation dialysis area?
No, it is not necessary. Essentially, a buffer zone is a potential contamination area. The potential contamination areas outlined in the “Hospital Isolation Technical Specifications” are located between clean and contaminated areas in respiratory infectious disease treatment areas and may be contaminated by patient blood, body fluids, and pathogenic microorganisms. This includes staff offices, treatment rooms, nurse stations, handling rooms for used patient items and medical equipment, and internal corridors, all of which belong to potential contamination areas. Infectious diseases in hemodialysis patients typically refer to hepatitis B, hepatitis C, AIDS, and syphilis, which are transmitted through blood, body fluids, secretions, and sexual contact, and occasionally through routine contact, but not through air or droplets. Therefore, it is unnecessary to establish a buffer zone between the regular dialysis area and the isolation dialysis area. What is important is that medical staff strictly implement hand hygiene protocols and adhere to environmental surface and air disinfection systems and other infection control measures in hospitals.
Q8: Can dry and wet storage rooms be in the same room?
It is best to have dry and wet storage rooms in different rooms. If they must be in the same room due to conditions, they should be set up in separate areas. The “Standard Operating Procedures for Blood Purification (2010 Edition)” states that storage rooms are a basic configuration of hemodialysis rooms, classified as clean areas for storing dialysis devices, tubing, puncture needles, and other consumables. They should be managed according to the Class III environment regulations outlined in the “Hospital Disinfection and Sanitation Standards.” The National Health and Family Planning Commission’s regulations on the management of hemodialysis rooms do not specify or require separate management of dry and wet storage rooms. Therefore, there is no explicit management basis for having separate dry and wet storage rooms in hemodialysis rooms. However, due to the variety and large quantity of consumables in hemodialysis rooms, most medical devices are in a dry state, while a small number contain a certain amount of water, such as dialysis fluid. If the packaging of water-containing medical devices is damaged or other unexpected situations occur, it can lead to dry medical devices becoming wet and contaminated.
Therefore, it is best to have dry and wet storage rooms in different rooms. If they must be in the same room due to conditions, they should be set up in separate areas. All medical devices should be placed on shelves to prevent water damage.
Q9: In the absence of a dedicated emergency dialysis machine, should emergency dialysis patients be placed in the regular dialysis area or the isolation dialysis area?
Since the maximum pore size of the dialysis membrane of the hemodialysis machine is only 3.5 nm, even the smallest viruses (diameter 18-22 nm) cannot penetrate the intact dialysis membrane. Moreover, since every component in the machine control unit does not have direct contact with the patient’s blood, bloodborne infectious diseases will not be transmitted through the hemodialysis machine or dialyzer when disposable dialyzers and tubing are used. Therefore, theoretically, it is possible to determine whether to set up dedicated emergency dialysis machines based on clinical work needs. Emergency dialysis patients use disposable dialyzers and tubing, and after dialysis, the machine is disinfected according to requirements. A properly disinfected hemodialysis machine is safe for use on other patients. However, due to the risk of bloodborne diseases being transmitted due to non-standard clinical operations, it is recommended to set up emergency dialysis machines, but they also need to undergo thorough disinfection after use.
Q10: After emergency hemodialysis patients use a dedicated emergency machine and test positive for bloodborne infection markers, how should the hemodialysis machine be disinfected?
Hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV) are all lipophilic viruses, which are the most sensitive microorganisms to various disinfectants, and low-level disinfection can kill them. According to the principles of hemodialysis, normally, even when treating infectious disease patients, the pathogens such as HBV, HCV, and HIV in the patient’s body will not penetrate the dialysis membrane into the internal circulation of the machine. In special cases of hemodialysis machine malfunction or rupture of the dialyzer membrane, these pathogens may enter the internal circulation pipeline, and after hemodialysis, heat-chemical disinfection of the hemodialysis machine can kill these pathogens, thus preventing the transmission of HBV, HCV, and HIV through hemodialysis.
While disinfecting the internal pipeline, the surfaces of the hemodialysis machine should also be cleaned and disinfected to prevent transmission through contact during work. Therefore, after emergency hemodialysis patients use a dedicated emergency machine and test positive for hepatitis B, hepatitis C, or AIDS markers, the hemodialysis machine should undergo internal heat-chemical disinfection and surface cleaning and disinfection, and after routine cleaning and disinfection, normal hemodialysis can be performed.
Q11: Can hemodialysis machines used by patients with bloodborne infectious diseases be disinfected and then used for regular patients? Can nurses in the isolation dialysis area perform procedures for patients in the regular dialysis area?
Theoretically, hemodialysis machines used by infectious disease patients can be effectively disinfected on the surface and internal pipelines and then used for regular patients. The reason why hemodialyzers can perform dialysis and eliminate toxins is that there are many micropores on the semi-permeable membrane of the dialyzer. Since these micropores are very small, no microorganisms, including viruses, can penetrate them. Therefore, theoretically, bloodborne infectious diseases such as hepatitis B, hepatitis C, AIDS, and syphilis cannot be transmitted through hemodialysis.
However, for hemodialysis patients, blood transmission is not the only route for infectious diseases such as hepatitis B, hepatitis C, AIDS, and syphilis. Contamination of dialysis unit surfaces, minor injuries to the skin and mucous membranes of dialysis patients, invasive procedures such as punctures for arteriovenous fistulas during hemodialysis, and blood exposure all increase the risk of infection for dialysis patients. To minimize the risk of infection for hemodialysis patients, management still requires segregated dialysis. Therefore, it is necessary to adhere to the regulations that bloodborne infectious disease patients must undergo hemodialysis in isolation areas, and hemodialysis machines used by infectious disease patients cannot be used for regular patients.
However, when regular patients need emergency dialysis and only hemodialysis machines used by infectious disease patients are available, it is necessary to weigh the pros and cons and choose the lesser of two evils.
As for the issue of whether nurses in the isolation dialysis area can perform procedures for patients in the regular dialysis area, the same reasoning applies. The original Ministry of Health’s “Standard Operating Procedures for Blood Purification (2010 Edition)” clearly states: hepatitis B and hepatitis C patients must undergo segregated dialysis and be equipped with dedicated dialysis operation supply carts, with nursing personnel relatively fixed. Management regulations must also be followed. However, in extremely special circumstances, such as in emergencies, medical staff can perform some procedures for other patients while strictly adhering to hand hygiene and other disinfection and isolation measures. Isolation dialysis is only one of the measures to prevent hemodialysis patients from being infected with bloodborne pathogens, not the only one; other disinfection and isolation measures must also be effectively implemented.
Q12: Can the touch screen of a hemodialysis machine be wiped with chlorine disinfectant?
It is recommended to refer to the user manual of the hemodialysis machine. If the manual does not mention it, consult the equipment manufacturer. Since the touch screen of the hemodialysis machine is frequently contacted during hemodialysis treatment, cleaning and disinfecting it after each hemodialysis treatment is very necessary. Proper cleaning and disinfection can effectively reduce the microbial load on the touch screen surface and eliminate the risk of pathogenic microorganism transmission.
If the user manual of the hemodialysis machine allows the use of chlorine disinfectants to disinfect the touch screen, or after consulting the equipment manufacturer, it is recommended to use a disinfectant wipe with an effective chlorine concentration of 500 mg/L (note: cleaning wipes soaked in chlorine disinfectant should be wrung out to remove excess disinfectant) for wiping. Disinfectant wipes or other compliant disinfectants can also be used for cleaning and disinfecting the touch screen of the hemodialysis machine. When the touch screen is contaminated with blood, body fluids, or secretions, it should be cleaned and disinfected immediately.
In special circumstances, various films can also be used to provide barrier protection for the touch screen of the hemodialysis machine.
It is particularly important: regardless of the method used for cleaning and disinfecting the touch screen of the hemodialysis machine, the cleaning and disinfecting cloth should be wrung out as much as possible to prevent liquid leakage into the machine during wiping, which could cause internal circuit short circuits or damage to the touch screen.
Q13: Can medical waste bins be placed in the dialysis area?
During the entire dialysis process, some medical waste will be generated, such as a small amount of used cotton swabs, dressings, etc., which can be placed in the medical waste bin configured on the treatment cart; additionally, each dialysis unit will be equipped with a flushing bucket for holding the flushing solution during machine setup and placing the tubing and dialyzer upon completion. This flushing bucket is not equivalent to a medical waste bin; the removed tubing and dialyzer will be immediately transported to the temporary medical waste container.
The hemodialysis center should set up a temporary medical waste storage room with larger medical waste bins for collecting infectious medical waste. Infectious medical waste generated during patients’ hemodialysis treatment can be temporarily stored in the storage room and collected regularly. If, for various reasons, the hemodialysis center does not have a temporary medical waste storage room, placing a medical waste collection bin in the hemodialysis treatment area for collecting medical waste generated during medical activities is also acceptable.
However, it should be noted that medical waste bins should have lids, be kept closed at all times, and have warning labels, and should be collected promptly when they reach three-quarters full.
Q14: Can curtains be hung in the hemodialysis room?
Yes, but management should be strengthened. First, the purpose of the curtains should be clarified. The purpose of hanging curtains in various rooms is generally to protect privacy and block excessive outdoor light, and the curtains in the hemodialysis room serve these two purposes. However, since the hemodialysis room is a medical area within a medical institution, there are some special management requirements for curtains. Curtains should be cleaned regularly to prevent dust accumulation from affecting the air quality in the hemodialysis room when pulling the curtains.
Moreover, if the curtains are visibly contaminated, they should be cleaned and disinfected immediately before reuse.
Q15: Do staff need to change shoes when entering the dialysis area? Do other personnel need to wear shoe covers when entering the hemodialysis room?
Staff members entering the hemodialysis area need to change into full protective shoes, while other personnel do not need to wear shoe covers when entering the hemodialysis room.
The “Standard Operating Procedures for Blood Purification (2010 Edition)” requires that patients change into slippers before entering the reception area and dialysis treatment room. Staff must change into work clothes and work shoes before entering the dialysis treatment room and treatment area. The change of shoes mentioned here is necessary for wearing work attire during work and is also a requirement for occupational protection of medical personnel to avoid contamination by blood, body fluids, and other infectious materials on non-work shoes during work. Therefore, both hemodialysis staff and hemodialysis patients must wear full protective shoes when entering the treatment room, rather than just shoe covers.
According to the original Ministry of Health’s “Standard Operating Procedures for Blood Purification (2010 Edition)” and the “Hospital Air Purification Management Regulations”, the hemodialysis room, along with the hospital’s general wards, mother-infant rooms, examination rooms, treatment rooms, dressing rooms, laboratories, emergency departments, and other departments, all belong to Class III environments, and their management requirements should be the same. Entering these departments and areas does not require additional dressing, shoe changes, or other sanitary processes, nor is there a need to wear shoe covers.
Studies have shown that there is no significant difference in the impact of wearing shoe covers versus not wearing them on the bacterial contamination of the air and surfaces in medical environments. Wearing plastic shoe covers does not reduce the occurrence of hospital infections. Eliminating disposable shoe covers can also reduce material management costs in departments, lessen the workload of medical personnel during the process of putting on and taking off shoe covers, and decrease the generation of hospital waste. The hemodialysis room can reduce the risk of hospital infections by reinforcing hand hygiene among medical personnel and strictly implementing environmental cleaning and disinfection measures.
Thus, personnel from other departments and functions in the hospital do not need to wear shoe covers when entering the hemodialysis room.
Q16: Should medical waste generated by hemodialysis patients in the isolation dialysis area be collected separately and marked?
Regardless of whether they are infectious disease patients or non-infectious disease patients, the handling process and management requirements for infectious medical waste generated during diagnosis and treatment are the same. They all need to be labeled for medical waste and handed over to the centralized disposal center for disposal. Therefore, medical waste generated by hemodialysis patients in the isolation dialysis area does not need to be collected separately or marked additionally.
It is important to note that according to current national regulations, household waste generated by infectious disease patients must also be collected using yellow special bags for infectious medical waste to reduce the risk of these high-risk infectious wastes leaking and contaminating during collection, temporary storage, and transportation.
Source and References:
[1] National Food and Drug Administration. Water Related to Hemodialysis and Treatment (YY 0572-2015) [EB/OL] (2015-03-02) [2017-04-07]
[2] Hu Bijie, Liu Ronghui, Liu Bin, et al. SIFIC Hospital Infection Prevention and Control Operational Atlas [M]. Shanghai: Science and Technology Press, 2015.
[3] Wang Zhigang. Blood Purification Studies [M]. Beijing: Science and Technology Press, 2013.
[4] Ministry of Health of the People’s Republic of China. Standard Operating Procedures for Blood Purification (2010 Edition) [EB/OL]. (2010-01-25) [2017-04-07]
[5] Hu Bijie, Liu Ronghui, Chen Wensen. SIFIC Hospital Infection Prevention and Control Clinical Practice Guidelines [M]. Shanghai: Science and Technology Press, 2013.
[6] Ministry of Health of the People’s Republic of China. WS/T 367-2012 Technical Specifications for Disinfection in Medical Institutions // National Health and Family Planning Commission’s Hospital Management Institute Hospital Infection Quality Management and Control Center. Compilation of Hospital Infection Management Documents (1986-2015). Beijing: People’s Health Press, 2015:
[7] Ministry of Health of the People’s Republic of China. GB 15982-2012 Hospital Disinfection and Sanitation Standards [S] // National Health and Family Planning Commission’s Hospital Management Institute Hospital Infection Quality Management and Control Center. Compilation of Hospital Infection Management Documents (1986-2015). Beijing: People’s Health Press, 2015: 125-137.
[8] Jia Jianxia, Jia Huixue, Zhao Xiuli, et al. The Role of Disposable Shoe Covers in Controlling ICU Hospital Infections [J]. Chinese Journal of Hospital Infection, 2009, 19(4): 407.
Source: Gao Gao Knowledge Related to Electrolyzed Water
Disclaimer: The article is a reprint, and the copyright belongs to the original author. The views expressed in the article only represent the author. If there are any inappropriate aspects, please contact.