1Introduction
Endoscopic surgical imaging is generally viewed on a monitor through images captured by a camera.
2Monitors
• 1. Cathode Ray Tube (CRT) Monitor
Most operating rooms use CRT monitors. • 2. Liquid Crystal Display (LCD) Screen

The recently introduced flat LCD screens have yet to replace traditional monitors. For surgeons, the image monitor is the last element in the imaging chain. For the other elements in this chain, the weakest link will determine the overall quality (the strength of a chain is equal to its weakest link, as the old saying goes).
3Basic Function Principles
• 1. Basic Function Principles • Image Presentation
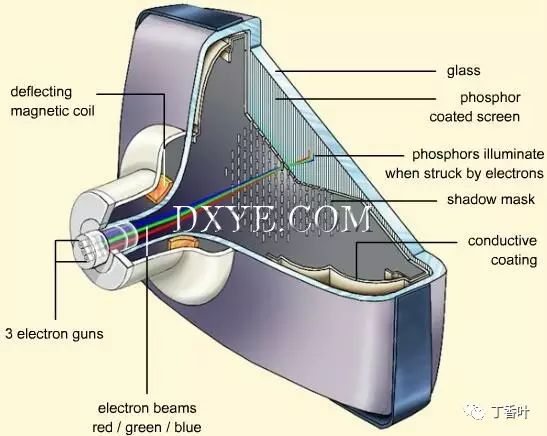
An image is presented on a CRT monitor screen by rapidly scanning continuous horizontal lines from top to middle, generated by three electron guns striking a phosphor-coated screen (a metal screen with many holes). • Types of Shielding
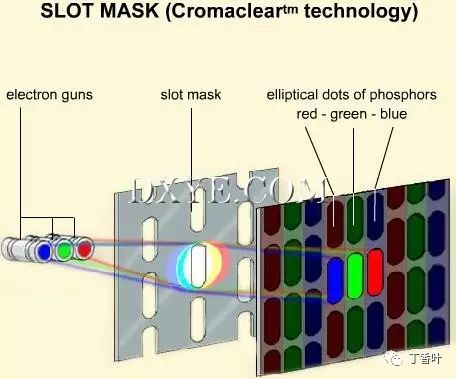

Each type of beam has a specific phosphor that, when struck, emits different colors: red, green, and blue (referencing RGB format). • Red, Green, Blue
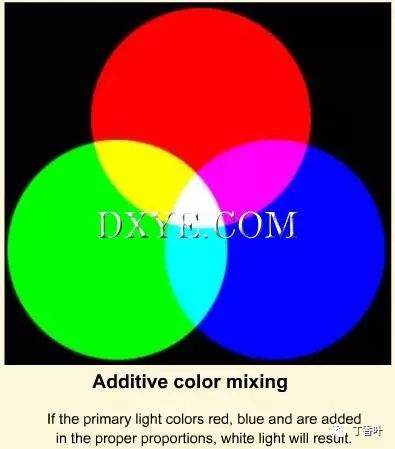
These three primary colors can be combined to produce the complete visible spectrum. The electron beam illuminates each phosphor point to generate the color of the image. • Standard Specifications
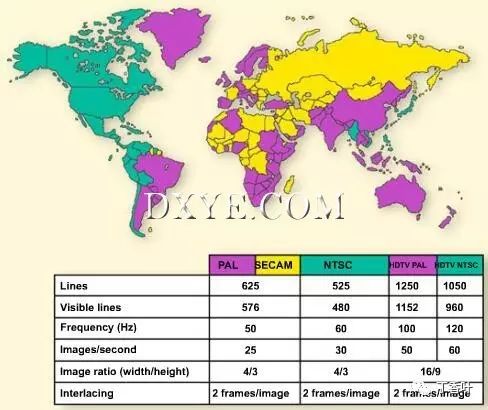
The European standard specification (PAL: Phase Alternate Line, SECAM: Séquentiel Couleur À Mémoire) and the American specification (NTSC: National Television System Committee) are different, but their principles are the same. • Interlacing
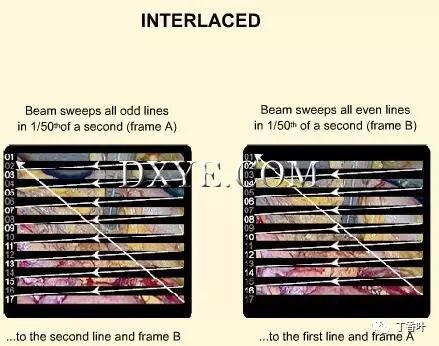
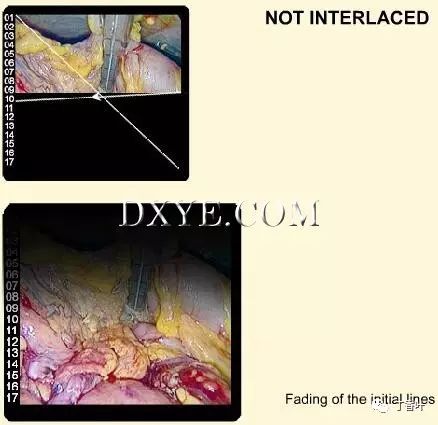
The CRT imaging system utilizes PAL, SECAM, and NTSC standards that are interlaced. Each frame consists of two fields presented by two passes. Initially, only one of the two horizontal lines is scanned from the top to the bottom of the screen (odd lines – odd field). Next, the other lines are scanned (even lines = even field). Thus, using the principle of interlacing, the entire screen will first display the first alternating line frame, then display the second frame to fill in the gaps left by the first. In Europe, the image refreshes at 25 times/second on a 50 Hz screen (it can refresh at 50 times per second). The frame rate is 1/25 frames/second for two interlaced frames resulting in 1/50 frames/second. The complete image (2 fields) is updated once every 1/25 seconds. Since the image is retained on the retina for about 1/30 seconds longer than the refresh rate, the brain cannot perceive individual frames but rather sees a complete image. Additionally, after the electronic impulse, the phosphor has a persistence effect that helps retain light for a time, allowing the brain to perceive a lasting image. The dual scan structure prevents screen flickering and enhances image clarity. Each range (odd and even) is equivalent to half of 312.2 line frames, thus producing a complete 625 line image (only 576 lines are used for the image, the remaining lines are for audio, synchronization, and other signals, such as television literary broadcasts). For progressive scanning, it means that before a frame appears, all lines of the previous frame are displayed from top to middle using interlacing, which is more accepted because when the scanning speed is insufficient, the first line may start to disappear when the beam reaches the midpoint. Regarding the NTSC standard, the operating system is entirely the same. The only difference is the number of horizontal scan lines and the frame refresh rate (due to the frequency of current oscillation). • 2. Cathode Ray Tube (CRT) Video Screen Resolution. • 100 Hz screens “100 Hertz” monitors used for surgical video screens typically utilize the 100 Hz version. This means that the image updates at a rate of 50 times/second, while the traditionally used screens update at a rate of 25 times/second. In other words, the frames are updated at double the frequency and speed. Therefore, the image will be smoother, less flickering, and reduce eye fatigue. • Resolution

The horizontal resolution of surgical video screens has doubled over the past decade and is now close to high-definition screens. The resolution of television screens depends on the number of horizontal scan lines (equivalent to the vertical resolution stipulated by the recording standard) multiplied by the number of vertical scan lines (equals horizontal resolution). This resolution depends on the number of pixels (phosphors) presented by any scan line, and therefore depends on the distance separating them. In fact, this refers to the maximum distance between vertical lines on a horizontal plane while distinguishing between white and black on the same plane. The closer these lines are to each other, the more lines can be seen on the surface of the screen. The horizontal specification of the screen is provided by its manufacturer, who measures it using test charts. For example, with a camera chain having 300 horizontal lines, 300 alternating dark lines and white spaces can be counted on the reference surface in the center of the screen. Most single CCD cameras have 400 horizontal resolution lines. However, the latest video cameras have 800 lines, sometimes even 900 horizontal resolution lines. Proper use of these lenses requires high-definition screens, which currently provide resolutions of 800 to 900 horizontal lines. As mentioned in the above specifications, HDTV (High Definition Television) screens provide over 1000 horizontal lines of resolution. However, it must be remembered that the vertical resolution (the number of horizontal lines) depends on the recording standard used (PAL = 625 lines, NTSC = 525 lines, HDTV PAL = 1250 lines, and HDTV NTSC = 1050 lines). • CRT Screen Models
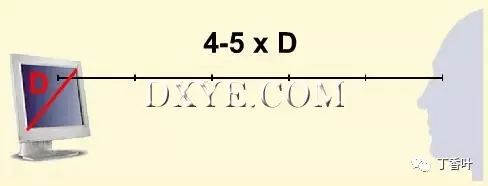
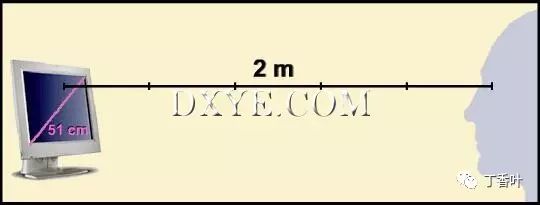
The model of the video screen is measured by its diagonal (including the screen frame). The most common diagonals are 36, 42, 51, or 63 centimeters (14, 17, 19, or 25 inches). In general, it is recommended to watch surgical videos from a distance of 4 to 5 times the screen’s diagonal. This is why it is suggested to use a 51 cm screen for laparoscopic procedures, as this type of screen allows the surgeon and surgical team to see clearly from a distance of 2.5 meters (8 feet). Using a smaller screen can lead to eye fatigue. • 3. Connections
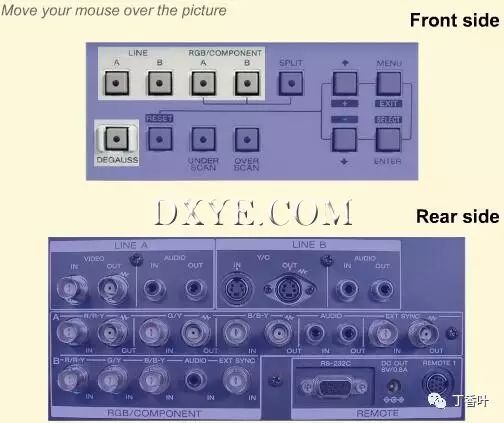
The connection between the video screen and the endoscopic camera is similar for compatibility. This is a composite connection (BNC); brightness (light intensity) and color are combined into a single signal, and the composite connection (Y/C and RGB) separates the parameters. It should be noted that new digital cameras have DVI (Digital Visual Interface) digital output, which can directly transmit a digital signal without the need for digital-to-analog conversion. This type of connection can only be used with digital screens (e.g., LCD). The following connections can appear on the back of the screen: – BNC (Bayonet Neill Concelman): television output; –Y/C = S-Video = S-VHS: two independent cables, one for light intensity, the other for color, and the other mixed (Y = brightness synchronization signal, C = color); – RGB (Red-Green-Blue): three BNC connectors of the same length, each carrying its primary color. Brightness is not transmitted but is combined from the three colors using the following formula: Y = 1: white = 0.3R + 0.59G + 0.11B; – RGB-S: a fourth cable transmits the image synchronization signal, used to synchronize different video devices. The quality of the transmitted image mainly depends on the connection used. From an electronic perspective, the quality of the image depends on the amount of data transmitted between the camera capturing the image and the screen receiving it, as well as the quality of signal processing. The worst quality is obtained from composite BNC connections, while the best quality is obtained from composite RGB connections. To achieve correct white balance and produce accurate and reliable colors, this is essential. However, in general, the resolution will be limited by the screen, resulting in no significant improvement compared to Y/C connections. It should be noted that if using RGB connections, the colors on the screen cannot be adjusted. • 4. Flat LCD Screens • 1
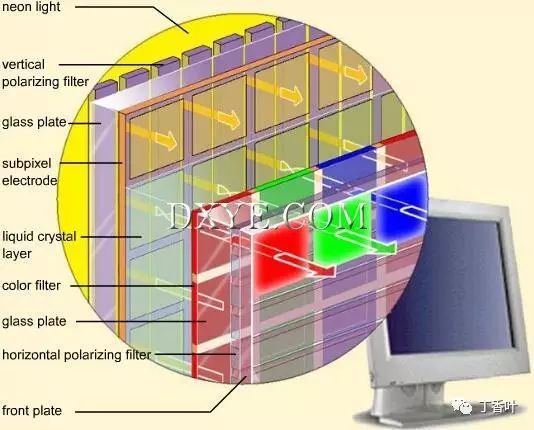
Compared to similar video screens, flat screens are digital computer screens. The two main types of LCD screens: – DSTN (Dual Scan Twisted Nematic) screens, more commonly known as passive matrix screens, meaning that each pixel (image element) is activated by a charge passing through a vertical cylinder and horizontal row control. When they meet, they unlock the pixels. – TFT (Thin Film Transistor) screens, also known as active matrix screens, where each pixel is controlled by its own transistor. Only TFT screens are used in operating rooms. The principles behind LCD technology are different from those behind CRT screens. Besides scanning the electron beam, there is a grid of liquid crystals clustered under RGB triads placed in front of a light source. • 2
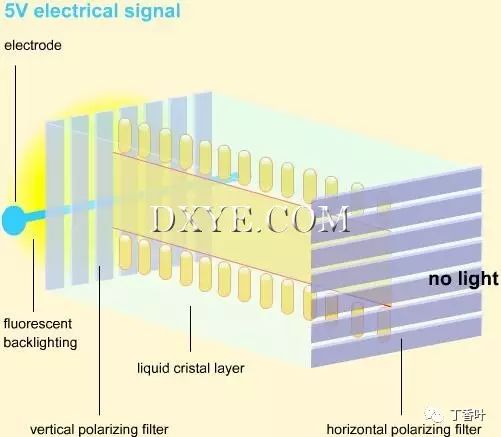
The characteristics of these liquid crystals are their linear structure and how they change direction when given an electric current. This property can modify the polarity of light. Then light can selectively pass through the liquid crystals. The resolution of these screens is not calculated by the number of scan lines but by the maximum display surface area. This corresponds to the actual number of pixels present on the grid (e.g., 1600*1200). Another parameter is the pitch; the distance between pixels is measured in centimeters. The lower the pitch, the closer the pixels are, increasing resolution. A good LCD monitor has a pitch of less than 0.28 centimeters. The refresh rate is not based on the AC frequency, but on the refresh frequency defined by the video signal (PAL = 25 images/second, NTSC = 30, HDTV PAL = 50, and HDTV NTSC = 60). LCD screens provide real advantages over CRT screens. Due to the absence of a cathode ray tube, they are generally brighter and less bulky. Their size is measured by the diagonal in inches, which corresponds to the actual viewing area. A 19-inch LCD screen is roughly equivalent to a 51 cm CRT screen. Another benefit is that the image is not scanned like a CRT monitor, so even when the viewer is close to the screen, it does not cause eye fatigue. Additionally, there is no direct electromagnetic radiation emitted, especially noticeable when close. Finally, the grid system composed of liquid crystals transmits the same quality of image to every point on the screen. As a result, the edges of the screen are no longer blurry or distorted. However, there are some drawbacks. Initially, the display quality is still poor. This is mainly due to the response time of each pixel. When the image changes rapidly, the viewer can perceive delayed images. Another major drawback involves the viewer’s angle. This is openly worse in passive matrix screens, as when the viewer is not directly in front of the screen, the image appears unattractive. Today, active matrix screens have made significant progress, with viewing angles exceeding 70 degrees, horizontally and vertically. In practical operation, as the viewer moves away from the center of the screen, the image quality continues to deteriorate. Moreover, LCDs are more difficult to produce black and dark gray. The conclusion is that LCDs generally have lower contrast and relatively reduced color saturation for low-intensity colors compared to CRTs. Finally, LCDs are more fragile than CRT screens. LCDs can sustain many weak or blocked pixels, and the damage is often irreparable. • 5. Plasma Screens • 1
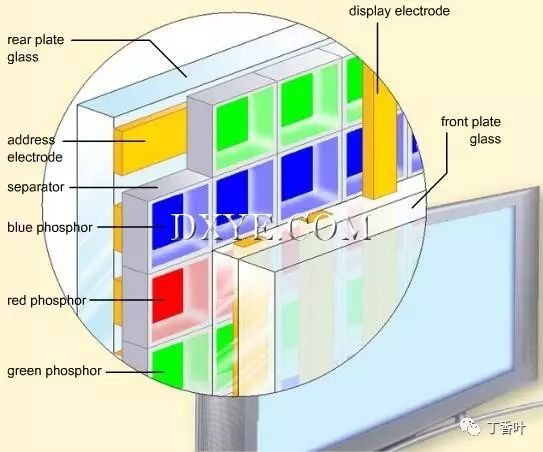
Plasma technology can produce wide, flat screens that provide a broad display (aspect ratio: 16:9). A plasma display consists of a layer of gas injected between two parallel glass panels, both covered by multiple rows of electrodes. When power is supplied, the gas reacts to produce ultraviolet light from the plasma. The ultraviolet light interacts with red, green, and blue phosphors at each image point to produce visible light. Unlike other imaging technologies, the image does not scan across the screen; in plasma technology…… • 2
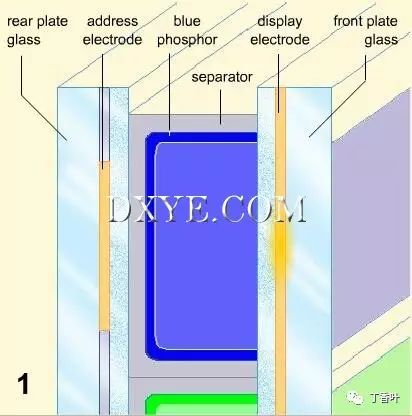
Plasma screens provide better image quality than LCD screens. However, the image quality of plasma screens still falls short of CRT screens, particularly in terms of color accuracy and contrast. Plasma screens are too large for standard operating rooms, and as of 2003, there was no plasma screen that met medical standards.
4Reasonable Requirements / Laparoscopy
To achieve ideal conditions for laparoscopy, a high-performance video system is essential.
Initially, many components of laparoscopy were equipped with screens utilizing 625 lines of vertical resolution (PAL standard) and 300 to 400 lines of horizontal resolution. Nowadays, CCD (computer-controlled display) sensors have made camera images perfect, so it is recommended to use screens with 800 to 900 lines of horizontal resolution. In principle, the resolution of the laparoscopic screen should be as close to the camera resolution as possible to prevent some avoidable signal degradation.
5Available Tools
Monitors are measured based on the diagonal of the screen, horizontal resolution, and adjustability. The screen should be calibrated according to the camera image. For standard laparoscopic surgery, it is recommended to use a 51 cm (19 inch) diagonal screen, a 100 Hz image refresh rate, and a screen with 800 horizontal resolution lines. These specifications can currently provide excellent images transmitted from endoscopic cameras.
6Usage and Adjustment
• 1. Installation
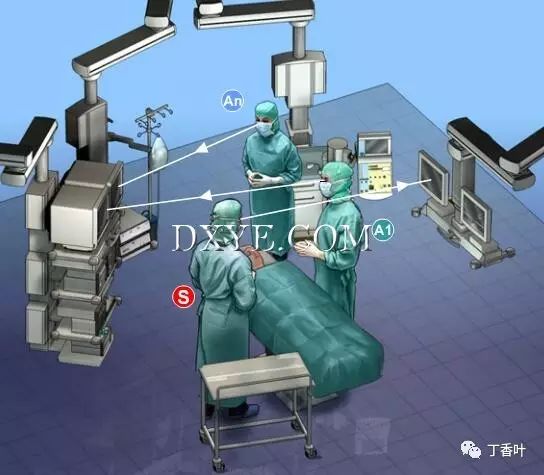
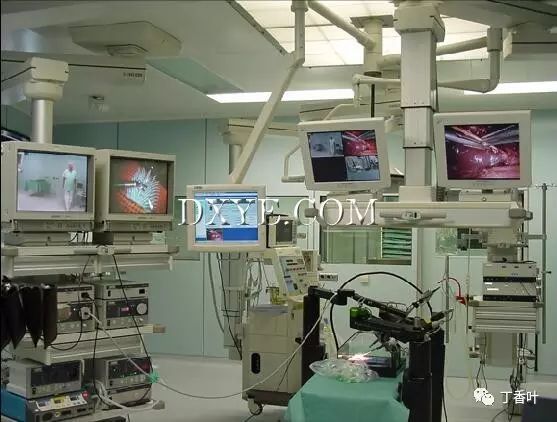
The installation of monitors in the operating room primarily depends on the frequency of laparoscopic use. Typically, monitors are placed on a set of laparoscopic components and moved along with other equipment. It is recommended to install a second monitor opposite the first to provide assistants with a good surgical view. Additionally, it allows the entire surgical team, including anesthesiologists, to closely observe every surgical step, regardless of their standing position. Logically, a third fixed monitor can be installed in a designated position in the operating room.
• 2. Lifespan Contrary to common belief, CRT monitors do not maintain good condition indefinitely. The arrangement of the electron beam scanning the screen gradually loses precision as it passes through the shielding. The electron guns gradually lose their power, and the phosphor layer on the screen also gradually changes, especially when a fixed image is displayed on the screen for a long time. One must consider that a video monitor used for over 6000 hours will no longer achieve its maximum effectiveness, and it should be noted that cathode ray tubes are designed to operate for about 20000 hours. Most users reach this lifespan after using the monitor for 3 to 6 years, as the monitor is usually illuminated for longer than its actual usage time. Therefore, the electron beam must be recalibrated by the manufacturer. If it has lost too much power or if the phosphor layer has changed, the monitor must be replaced.
• 3. Color Temperature
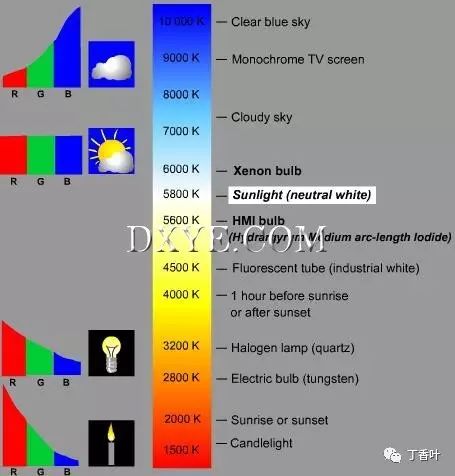
As mentioned in the sections on cold light sources and cameras, adjustments made in the video series must match the color temperature of the cold light source. Currently, surgeries typically use metal halide lamps or xenon arc lamps, with color temperatures between 5600 and 6000 Kelvin (K). Most video screens are set at around 6500K. Once verified, no special adjustments are needed. The color temperature setting for computer screens is higher (9500K), so adjustments are required. These adjustments can usually be made through the selection menu on the screen (refer to the manufacturer’s user guide).
• 4. Related Adjustments
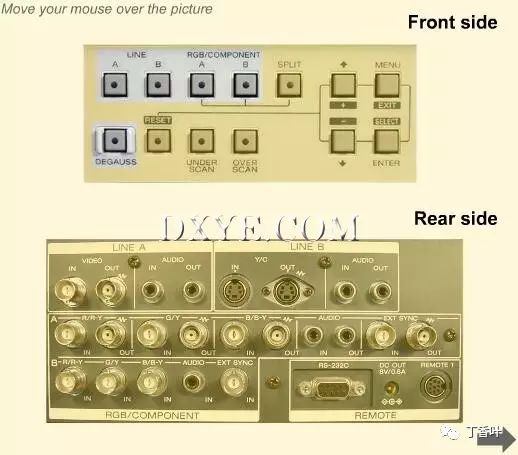
Related adjustments for CRT monitors: Most monitors have the same adjustment systems: – Color or chrominance: Adjusts the overall color of the image. If this screen is connected to an RGB source, this adjustment is ineffective. – Phase: Makes red appear purple or green (only effective on non-RGB and NTSC standards). – Contrast: Modifies the difference between the darkest and brightest parts of the image. It can also adjust color reproduction and display. – Aperture: Smooths or sharpens the outline of the image. If there is text on the screen, the effect of the adjustment is more pronounced, but if connected to RGB, it cannot be operated. – Demagnetization: Can demagnetize the CRT when a bad magnetic field distorts the image or colors. The screen will automatically demagnetize after restarting. This occurs automatically after being powered on. And it cannot be demagnetized again within at least 10 minutes after the last demagnetization. – Input Selector (A, B, RGB line): Selects the signal from the connection that corresponds to the video source being used (BNC, Y/C, RGB).
7Usage Issues

Aside from the total disappearance of the image caused by the electron beam fading, the monitor will only be affected by certain changes. The main anomalies are caused by the monitor being placed too close to electromagnetic sources or metallic objects. This will cause the electron beam on the screen to deviate from its path, producing a color fringe, mostly green. The solution is to move the screen away from the source of electronic deviation. If there are changes in display, the monitor must be returned to the manufacturer for confirmation and recalibration. If the problem stems from a defect in the cathode ray tube, it must be replaced. Due to the high cost of repairs, the entire monitor set is generally replaced.
8Conclusion
As the final element in the imaging chain, monitors are often the boundary determining factor of the entire chain and should not be neglected. Their quality and resolution must be equivalent to that of the camera to provide the surgeon with the most ideal visual comfort.
