
After the pandemic, the pressure on hospital emergency rooms has increased significantly. On one hand, infectious diseases such as influenza and dengue fever are recurring, coupled with a surge in chronic diseases like heart disease and diabetes due to an aging population, leading to more people visiting hospitals; on the other hand, there is a severe shortage of nurses.——The World Health Organization states that by2030, the global shortage of nurses could reach13 million. This has resulted in emergency rooms often being overcrowded, with patients waiting too long, and some even leaving before being seen.
To alleviate this issue, there has been a push to haveAI assist in performing“triage”—that is, quickly determining which department a patient should go to based on their symptoms. However, currentAI triage systems often encounter problems. A research team from South China University of Technology has designed a“multi-agent collaborative system” to allow severalAI roles to work together, making triage both fast and accurate. The paper titled“Collaborative Medical Triage under Uncertainty: A Multi-Agent Dynamic Matching Approach” details how this system works.
In fact, the problem this paper aims to solve has already been addressed by Baidu Health, which developed and launched a similar triage robot using achatBot+Agent model during the period of2024-2025, and it has been implemented in top hospitals like Wuhan Union Hospital, even going online across the board as the first point of contact for hospitals and patients, receiving high praise from both hospital and government sides. In addition to the efficiency and accuracy improvements mentioned in this paper,AI triage also has the following benefits: it enables automatic and fair appointment allocation, placing patients with complex conditions who require specialized doctors into the queues of authoritative physicians; it bridges data silos in hospitals such asHIS, so that all basic information and test results appear directly on the doctor’s workstation before the patient meets the doctor; it avoids awkwardness and privacy issues in information collection, such as male patients feeling shy when answering sensitive questions from female doctors, which can largely be alleviated through dialogue withAI.
1. The Three Major Pitfalls of ExistingAI Triage Systems
Currently, many hospitals or platforms are experimenting withAI triage, such as using large models likeGPT to analyze the symptoms described by patients and recommend departments. However, in practice, there are numerous issues, which can be summarized into three“pits”.
The first pit is“lack of professionalism, leading to random recommendations”. Although large models can articulate well, they sometimes experience“hallucinations”—that is, they fabricate non-existent medical knowledge. For example, if a patient says“I have a headache”, an untrainedAI might randomly recommend going to the“neurosurgery department”, when in fact it is more likely a problem for the“neurology department”, and such random recommendations could delay treatment.
The second pit is“inability to adapt to different hospital department setups”. Large hospitals have very detailed department divisions; for example, there are pancreatic surgery and vascular surgery departments, while smaller hospitals may only have a“general surgery department”. CurrentAI systems either need to be retrained for each hospital (which is too costly) or use generic data (leading to inaccurate recommendations). It’s like using a“supermarket product classification table” for all supermarkets—large supermarkets have sections for“snacks, beverages, and fresh produce”, while small supermarkets might only have“food and household items”, which is definitely not suitable.
The third pit is“asking too many irrelevant questions, slowing down the process”. Triage emphasizes“speed”, but currentAI systems tend to ask for excessive details. For instance, if a patient says“I have a fever”, theAI might repeatedly ask“What is the exact temperature? How long have you had the fever? How much does your temperature change each hour?”—in fact, these details are not that important for determining which department to go to, and they only make the patient wait longer.
2. ThreeAI Agents Collaborate to Turn Triage into a“Production Line”
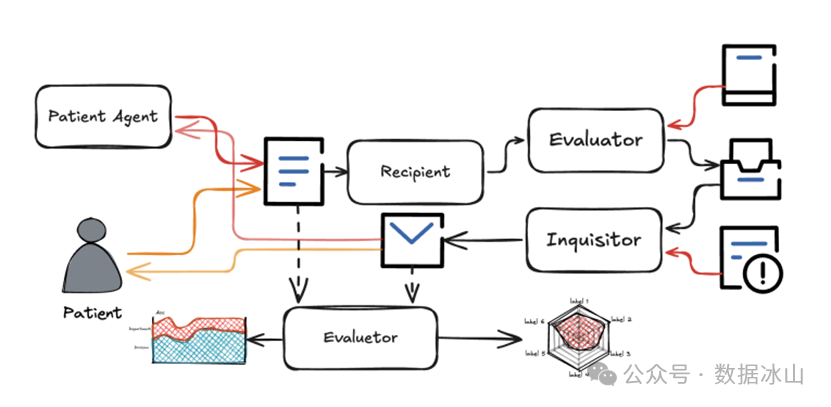
The team from South China University of Technology came up with a solution: instead of having oneAI do everything, they let threeAI roles collaborate, similar to a“three-person team” at a hospital triage desk.
The first role is called“Recipient Agent”. The symptoms described by patients are often very scattered, for example,“I had a headache this morning, feeling a bit dizzy, and the previous doctor asked me if I was vomiting”. ThisAI is responsible for organizing these statements into a“standardized medical record”—according to medical norms, clearly stating when the symptoms started, their characteristics, and what was previously asked. It’s like a front desk organizing a visitor’s various requests into a clear table for easier processing by others.
The second role is called“Inquirer Agent”. After receiving the standardized medical record, it will identify the missing key information. For example, if the medical record only states“headache” without mentioning“whether there is accompanying vomiting”, it will ask the patient targeted questions. However, it has a rule: it does not ask repetitive or irrelevant questions. For instance, to determine“whether the headache should go to neurology or neurosurgery”, the key question is“whether there has been any trauma”, so it will only ask that and not get bogged down with secondary questions like“Does your vision blur when you have pain?”.
The third role is called“Department Agent”. It recommends which department to go to based on the complete medical record and the hospital’s department list. For example, if a large hospital has“neurology” and“neurosurgery”, it will check if the patient has any trauma—if there is trauma, it will recommend neurosurgery; if not, it will recommend neurology. If it is a small hospital with only“internal medicine”, it will directly recommend internal medicine. It’s like a triage doctor using the hospital department list to make judgments while avoiding easily confused departments.
These threeAI agents do not work independently; they collaborate in rounds. For example, in the first round, after the patient describes their symptoms, the“Recipient Agent” organizes the medical record, the“Department Agent” finds that the information is insufficient, and the“Inquirer Agent” will ask follow-up questions; in the second round, after the patient responds, the“Recipient Agent” updates the medical record, and the“Department Agent” reassesses… up to four rounds, an accurate recommendation can be provided.
To make the system adaptable to different hospitals, the team also designed a“guidance rule library”. Each department has its own“judgment points”; for example, internal medicine might ask“Do you need medication?”, while surgery might ask“Is there any trauma?”. Large hospitals load more detailed rules, while small hospitals load simpler rules, eliminating the need to retrain theAI—just modifying the rules is sufficient, which significantly reduces costs.
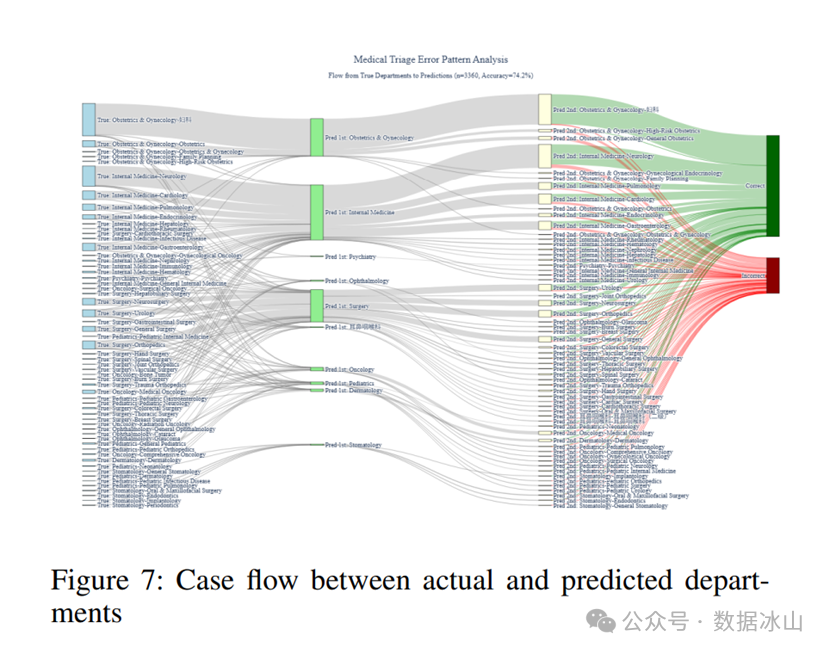
3. Testing with 3360 Real Cases: Accuracy Reaches89%
To validate their approach, the team sourced3360 real cases for testing—these cases came from the“Ai Ai Yi” platform, covering9 primary departments (such as internal medicine and surgery) and62 secondary departments (such as neurology and gastroenterology), which can represent the needs of different hospitals.
The results were significant: after four rounds of interaction, the accuracy of recommendations for primary departments reached89.2%, while for secondary departments it reached73.9%. Moreover, the accuracy increased with each round—accuracy for the first round of primary departments was85.5%, and by the fourth round, it had increased by nearly4 percentage points. This indicates that multi-round collaboration is indeed effective, asAI can continuously correct its judgments through follow-up questions.
They also specifically tested“what happens if one role is removed”. For example, if the“Recipient Agent” is removed and the otherAI agents are left to judge based on the patient’s original dialogue, the accuracy dropped by33%. This is akin to not having a front desk to organize information, leaving the inquirers and recommenders with a jumble of scattered statements, making it impossible to work effectively.
Additionally, the system not only looks at accuracy but also scores on six dimensions: whether the inquiry was focused, whether the recommendation was correct, whether the reasoning was logical, whether the communication was clear, whether there were contradictions in multi-round interactions, and whether the overall professionalism was sufficient. The final average score was3.65 (out of a maximum of5), with the highest score for“recommendation accuracy” (4.25), indicating that it can indeed assist in clinical settings.
4. A Challenge for Investors: Can Implementation Costs Really Be Reduced?
This system sounds promising, but for investors, the most concerning question is“can it be implemented at a low cost?” The paper claims it is cheaper than traditional“large model fine-tuning” because it only requires modifying the rule library without retraining the model. However, there is a problem: the departmental rules of different hospitals can vary greatly; does organizing these rules require a large number of doctors to participate? If a small hospital lacks the capability to modify the rules, will it still need assistance from the team? In the long run, will the maintenance costs of these rules be higher than expected?
If entrepreneurs claim“we can quickly adapt to any hospital”, it might be worth asking:“Have you tested this in more than three hospitals of different scales (such as tertiary, secondary, and community hospitals)? How many days does it typically take from obtaining the hospital department list to having the system operational?”—the real challenges of implementation often lie in these details.
5. A Reminder for Entrepreneurs: What About Rare Diseases?
The system currently uses3360 cases, most of which are common diseases. However, in actual triage, there may occasionally be rare diseases, such as“abdominal purpura” (a rare type of abdominal pain), which has symptoms similar to ordinary gastroenteritis but requires a completely different department recommendation. If the system has never encountered such cases and the rule library lacks relevant judgment standards, it may make incorrect recommendations.
At this point, one must consider: should the system have a“manual intervention switch”? For example, whenAI detects“this combination of symptoms has never been seen before”, should it automatically alert a nurse to intervene? Or can the system be designed to“learn on the go”, automatically updating the rule library when encountering new cases? After all, the biggest fear in the medical system is not“not doing well enough”, but“being confidently wrong”.
Conclusion: MakingAI Triage as Reliable as an“Experienced Nurse”
Overall, the concept of this multi-agent system is quite ingenious—it does not rely on a singleAI” to work alone, but rather on collaborative division of labor, with each agent performing its role. It resembles an experienced triage team in a hospital: the front desk records information, nurses ask for key details, and doctors make departmental judgments, working together to be both fast and accurate.
More importantly, it addresses the core contradiction ofAI in medical scenarios: it needs to be professional and accurate, yet flexible enough to adapt to different institutions, while also being efficient and time-saving. If it can be tested and refined in more hospitals in the future, it may indeed help relieve the pressure on emergency rooms, reduce patient wait times, and lessen the burden on nurses. This is likely the most tangible value ofAI in the medical field.