CRP is an acute phase protein synthesized by liver cells in response to inflammatory stimuli such as microbial invasion or tissue damage.
The acute phase response includes changes in the concentration of certain serum proteins during infection, inflammation, and trauma. These proteins, in addition to CRP, include serum amyloid A, fibrinogen, haptoglobin, α1-acid glycoprotein, ceruloplasmin, and α1-antitrypsin.
In healthy individuals, the concentration of CRP in serum is very low (<5mg/L), but it significantly increases during bacterial infections or tissue damage, hence it is considered most valuable.
1
Normal Reference Values
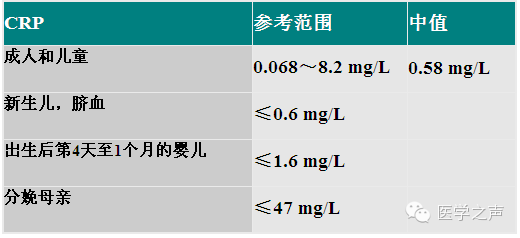
Image Source: Voice of Medicine
2
What Can It Reflect?
1. Screening for organic diseases;
2. Acute or chronic inflammation, such as with bacterial infection;
3. Autoimmune or immune complex diseases;
4. Tissue necrosis and malignant tumors.
01
Diagnosis and Differentiation of Infections
CRP begins to rise 6-8 hours after bacterial infection, peaks at 24-48 hours, and rapidly decreases after the infection is resolved, returning to normal within a week.
Gram-negative bacterial infections: can cause the highest levels of CRP, sometimes reaching 500mg/L;
Gram-positive bacterial infections and parasitic infections: typically cause a moderate response, usually around 100mg/L;
Viral infections: CRP does not significantly increase during viral infections; the response is mild, usually not exceeding 50mg/L, and rarely exceeds 100mg/L;
-
During the acute phase of bacterial infection, CRP significantly increases while oligoadenylate synthetase remains normal;
-
During viral infections, CRP levels are normal or slightly elevated, while oligoadenylate synthetase levels increase.
02
Predicting Future Risks of Myocardial Infarction and Stroke
-
C-Reactive Protein is the strongest risk indicator for cardiovascular diseases, and CRP levels can predict the risk of future myocardial infarction and stroke.
Individuals with C-Reactive Protein levels >2.1mg/L compared to those <1mg/L:
Have a 2.9 times higher risk of myocardial infarction;
Have a 1.9 times higher risk of ischemic stroke;
Have a 4.1 times higher risk of peripheral vascular disease.
-
Within hours after pain onset, CRP rises, peaks at 3-4 days, and returns to normal 7-10 days after CK-MB normalizes.
03
Autoimmune or Immune Complex Diseases
-
In systemic lupus erythematosus, polymyositis, and systemic sclerosis, CRP shows no significant changes, thus it can be used to differentiate from rheumatic diseases;
-
Fever may indicate a concurrent infection rather than a worsening of the disease.
04
Cancer
-
Elevated or rising CRP indicates poor prognosis and often suggests metastasis;
-
Colorectal cancer is the second leading cause of cancer-related deaths. Studies show that individuals with the highest blood C-Reactive Protein levels are twice as likely to develop colorectal cancer compared to those with the lowest levels.
05
Assessing Disease Activity and Monitoring Treatment Efficacy
-
CRP levels of 10-50mg/L indicate mild inflammation;
-
CRP rising to 100mg/L indicates more severe disease, and its severity may require intravenous injection;
-
CRP > 100mg/L indicates a severe disease process and often suggests the presence of bacterial infection.
06
Monitoring Antibiotic Treatment
Serial measurements of plasma CRP can be used for treatment monitoring in the following situations:
-
Effective use of antibiotics during many infections;
-
Adjusting anti-inflammatory drug dosages based on changes in CRP levels;
-
Discontinuing antibiotic treatment when CRP returns to normal;
-
Guiding antibiotic treatment in high-risk populations where microbiological diagnosis is lacking.
07
Surgery
-
CRP levels significantly increase 24-72 hours after surgery, returning to normal around days 5-7;
-
Persistent high levels after a sharp rise often indicate concurrent infection;
-
For patients undergoing medium to large surgeries, routine testing should be done preoperatively and 3-7 days postoperatively;
-
For those with CRP still high 5-7 days post-surgery, concurrent infection should be suspected, and follow-up monitoring should be conducted.
08
Internal Medicine
Pneumonia
CRP >100mg/L strongly indicates bacterial infection, such as purulent bronchitis or pneumonia; typical viral pneumonia does not exceed 50mg/L;
Cardiovascular Diseases
CRP rises within hours after pain onset, peaks at 3-4 days, and returns to normal 7-10 days after CK-MB normalizes.
Metabolic Syndrome
Metabolic syndrome can be classified based on CRP levels:
Low-risk group: <1mg/L;
Medium-risk group: 1-3mg/L;
High-risk group: >3mg/L.
09
Obstetrics and Gynecology
-
Pelvic inflammatory disease and adnexitis show elevated CRP levels;
-
Pelvic masses and uterine fibroids are usually negative;
-
Diagnosis of intrauterine infection in cases of premature rupture of membranes;
During premature rupture of membranes, if the mother’s CRP exceeds 50mg/L within 6-19 hours before delivery, it can be used as a criterion for the occurrence of in situ adenocarcinoma (AIS); CRP observed on the first day postpartum will be 2-3 times higher than in normal deliveries.
-
Uncomplicated CT and NG infections do not cause CRP elevation. However, if they spread to the pelvis, an acute phase response may occur.
10
Pediatrics
Neonatal Sepsis
CRP >10mg/L within 3 days after birth indicates infection;
If CRP does not exceed 10mg/L within 24 hours, there is likely no neonatal infection.
Fever in Children
If illness exceeds 12 hours, CRP significantly >40mg/L, and erythrocyte sedimentation rate (ESR) significantly >30mm/h, bacterial infection should be suspected.
Meningitis
CRP >20mg/L suggests the possibility of bacterial infection;
At >100mg/L, it has diagnostic value for bacterial infection;
In cases of meningitis, CRP between 20-60mg/L, successful treatment can reduce CRP to normal within a week.