Diuretics are the cornerstone of heart failure treatment. What are the commonly used diuretics? What are their characteristics? At the 15th Qianjiang International Cardiovascular Disease Conference, Professor Mao Wei from the Zhejiang Provincial Hospital of Traditional Chinese Medicine gave an excellent presentation on these questions!
Recommended Common Diuretics
Professor Mao Wei mentioned that the 2018 heart failure guidelines in China categorize diuretics mainly into two types: sodium excretion and water excretion. Among them, water-excreting diuretics are mainly tolvaptan, while sodium-excreting diuretics are divided into loop diuretics, thiazide diuretics, and potassium-sparing diuretics.
Additionally, Professor Mao pointed out the differences between the guidelines for diuretics in China and European countries:
In the recommendation of loop diuretics, the recommended dosage of furosemide in China is lower than that in the European guidelines, while the recommended dosage of torsemide is higher than that in the European guidelines;
In the recommendation of thiazide diuretics, the European guidelines include bendroflumethiazide;
In the recommendation of potassium-sparing diuretics, spironolactone is not classified as a diuretic in China, while in the ESC guidelines, spironolactone/eplerenone is included in both neurohormonal inhibitors and diuretics, and the AHA guidelines recommend spironolactone as an oral diuretic.
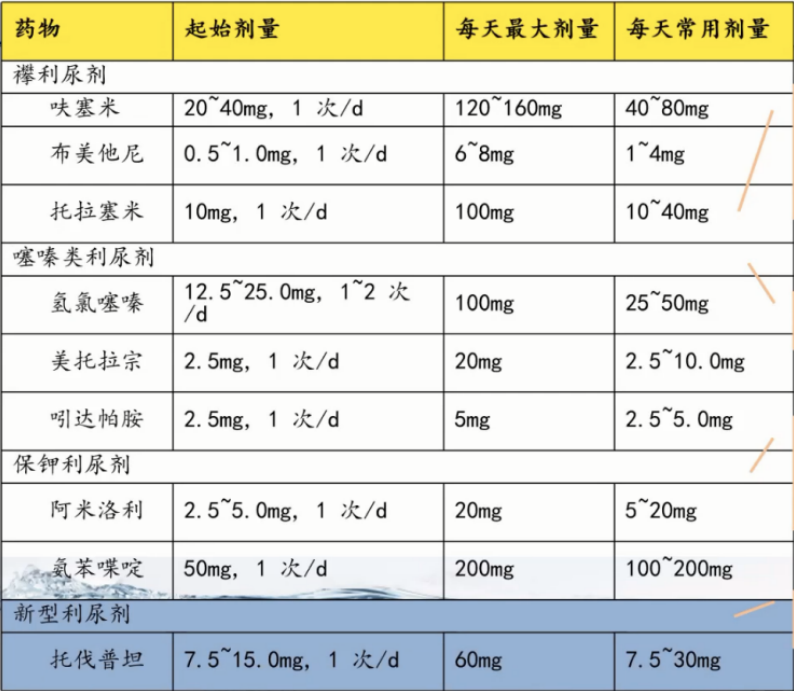
Figure 1. Recommended Diuretics in the 2018 Heart Failure Guidelines in China
Characteristics of Various Diuretics
Professor Mao then explained the characteristics of loop diuretics, thiazide diuretics, potassium-sparing diuretics, and various new diuretics.
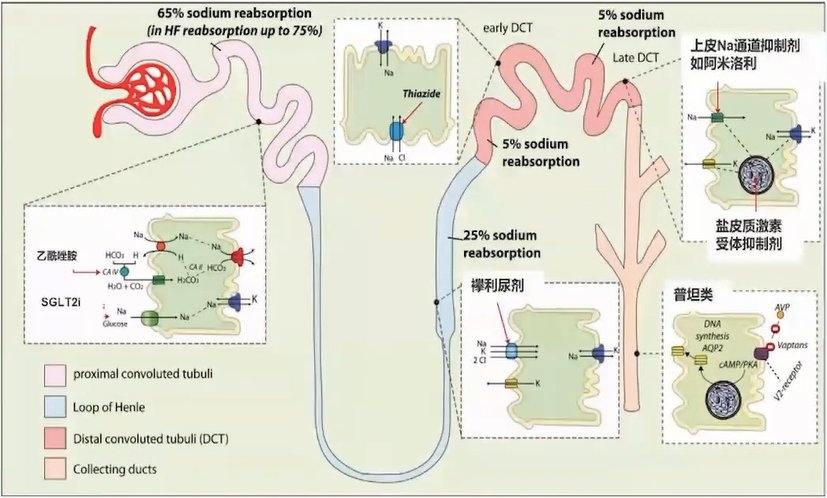
Figure 2. Action Targets of Different Diuretics
1. Loop Diuretics
Suitable for most heart failure patients, especially those with significant fluid retention or impaired renal function, including furosemide, torsemide, and bumetanide.
The dosage of loop diuretics has a linear relationship with the effect, and patients with severe renal impairment [eGFR < 15 mL/(min·1.73 m²)] need to increase the dosage.
40 mg of furosemide, 20 mg of torsemide, and 1 mg of bumetanide have comparable diuretic effects.
When there is no severe renal impairment, the diuretic effect of furosemide injection is equivalent to twice that of the oral form (i.e., intravenous furosemide 10 mg = oral furosemide 20 mg);
However, due to the higher oral bioavailability of torsemide and bumetanide (80%-100%), which is less affected by intestinal congestion, the efficacy of intravenous and oral forms is similar.
Furthermore, Professor Mao emphasized that loop diuretics are threshold drugs, meaning that a threshold concentration must be reached for diuretic effects. As blood drug concentration increases, the diuretic effect presents an S-shaped curve, reaching a plateau at commonly used doses.
In patients with acute decompensated heart failure (ADHF), the concentration-effect curve of diuretics shifts to the right, with the maximum effect plateau decreasing and the diuretic threshold increasing.
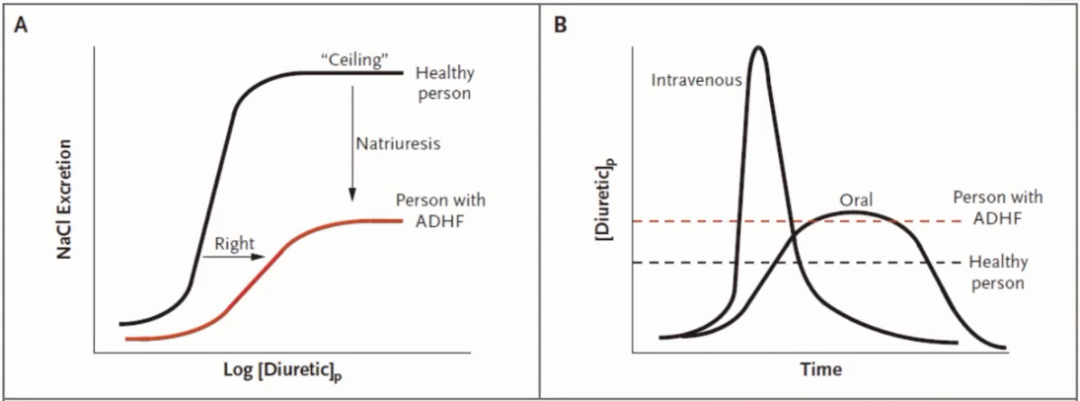
Figure 3. Pharmacokinetic Characteristics of Loop Diuretics
2. Thiazide Diuretics
Thiazide diuretics have a weaker diuretic effect compared to loop diuretics and are only suitable for heart failure patients with mild fluid retention and normal renal function.
Hydrochlorothiazide 100 mg/d has reached the maximum effect (the dose-effect curve has plateaued), and further increases are ineffective.
Additionally, in patients with renal impairment [eGFR < 30 mL/(min·1.73 m²)], the effect of thiazide diuretics is diminished and their use is not recommended; however, in patients with refractory edema (furosemide daily dose > 80 mg), thiazide diuretics can be combined with loop diuretics.
3. Potassium-Sparing Diuretics
Amiloride and triamterene have weak diuretic effects and are generally used in combination with other diuretics. Aldosterone receptor antagonists are also potassium-sparing diuretics.
Clinically, non-diuretic doses of low-dose aldosterone receptor antagonists are mainly used to improve myocardial remodeling, such as spironolactone 20 mg or eplerenone 25-50 mg.
To achieve diuretic effects, high doses of aldosterone receptor antagonists are needed, such as 50-100 mg of spironolactone. Eplerenone is a selective aldosterone receptor antagonist with minimal effects on sex hormone receptors and fewer side effects.
4. Vasopressin V2 Receptor Antagonists
The representative of the vasopressin receptor antagonists is tolvaptan. Tolvaptan does not need to be secreted into the renal tubular lumen to exert its effect, increasing its efficiency, and its diuretic effect does not depend on blood sodium and albumin levels.
Tolvaptan is significantly effective for patients with refractory edema or hyponatremia, and it remains effective for high-risk groups such as the elderly, hypotensive patients, those with hypoproteinemia, and renal impairment.
It is recommended for patients who do not respond well to conventional diuretic treatment and have hyponatremia or a tendency toward renal impairment. Moreover, its main side effect is hypernatremia.
Optimizing Treatment
1. Patients with Acute Decompensated Heart Failure (ADHF)
Should maintain a negative fluid balance of about 500-5000 mL/d based on water and sodium retention, gradually transitioning to a balanced intake and output. For patients with significant pulmonary congestion, systemic congestion, and edema, strict water and intravenous fluid rate restrictions should be implemented.
For those without obvious hypovolemia (massive bleeding, severe dehydration, excessive sweating, etc.), the daily fluid intake is generally within 1500 mL, maintaining a negative balance of about 500 mL daily.
For patients with severe pulmonary edema, the water negative balance can be 1000-2000 mL/d, and in severe cases, it can reach 5000 mL/d, transitioning to a gross balance after 3-5 days. At the same time, sodium intake should be limited to < 2 g/d.
For patients with ADHF with low perfusion, diuretics should be avoided until adequate perfusion is achieved.
2. Combined Diuretic Resistance
Professor Mao pointed out that the following methods can be used to address this:
• Increase the dose of loop diuretics;
• Change the route of administration (intravenous push combined with continuous intravenous infusion: continuous and multiple intravenous applications can avoid sodium and water reabsorption due to decreased loop diuretic concentration);
• Use two or more diuretics in combination, such as adding thiazide diuretics on top of loop diuretics, or adding vasopressin V2 receptor antagonists;
• Use medications that increase renal blood flow, such as low-dose dopamine or recombinant human natriuretic peptide, to improve diuretic effects and renal function, and enhance renal perfusion, but the benefits are unclear;
• SGLT2 inhibitors;
• Correct hypotension, hypoxemia, metabolic acidosis, hyponatremia, hypoproteinemia, infections, etc., especially pay attention to correcting hypovolemia;
• Ultrafiltration therapy
Summary
At the end of the conference, Professor Mao summarized the following four points:
1. Diuresis is the fundamental treatment for volume overload in heart failure;
2. Early combination of loop diuretics + tolvaptan + nesiritide;
3. SGLT2 inhibitors can provide osmotic diuresis while lowering blood sugar, reducing blood pressure, and decreasing cardiac preload, and are expected to become an effective option for patients with HFrEF/HFpEF with diuretic resistance;
4. If all diuretic strategies fail, consider ultrafiltration.
Layout: ly
Submission: [email protected]
Image sources in the text: Speaker PPT
This article was first published on the professional platform under Dingxiangyuan: Cardiovascular Time