“The Late Spring Festival”!
In 2020, as the Mid-Autumn Festival coincided with National Day, each person’s feelings and reflections on the tumultuous past six months and the sense of loss and recovery are countless. As families reunite, let us together remember the past and cherish the present!
The National Day holiday is already halfway through. According to the website of the Ministry of Culture and Tourism, from October 1 to 4, the country received a total of 425 million tourists, generating tourism revenue of 312.02 billion yuan.


The field of radiation oncology will benefit from standardized naming conventions for target areas, normal tissue structures, and treatment planning concepts and metrics. The AAPM 263 working group provides standardized naming guidelines for clinical trials, data aggregation, population studies, and routine clinical treatment in the field of radiation oncology.
The Significance of Standardized Naming for Radiation Oncology Structures:
1. Provides templates for initial subsets for clinical trial groups and user software platforms, offering naming patterns for other structures that may be included in the future;
2. Facilitates database development, automatic analysis of DVH metrics, and data exchange between institutions;
3. Promotes effective communication among all participants in clinical trials; common terminology can improve patient data exchange capabilities across multiple healthcare institutions;
4. Common terminology can provide a foundation for developing automated software tools and for automated extraction and analysis of data, submission, and data exchange; it can facilitate the implementation of automated QA processes;
5. Provides a framework for machine learning applications’ concepts and interrelationships;
1. Target Structure Naming Suggestions
The survey results of target structure naming members show that a very complex set of concepts is currently in use clinically: when several structures, doses, underlying structures, imaging modes, etc., exist, methods for classifying and enumerating the primary and lymph node target areas using ICRU and others emerge. Clinically, not all concepts are attempted to be represented; only some of the most important features are chosen for naming.
1/ The first group of characters must be one of the allowed target area types:
GTV
CTV
ITV
IGTV (Internal Tumor Volume – Consider Motion)
ICTV (Internal Clinical Target Volume – Consider Motion)
PTV
2/ When classifying target areas, place the target area classification symbol after the target area type, with no spaces. The target area classifications are as follows:
n: Lymph Node (e.g., PTVn)
p: Primary (e.g., GTVp)
sb: Surgical Tumor Bed (e.g., CTVsb)
par: Parenchyma (e.g., GTVpar)
v: Venous Thrombosis (e.g., CTVv)
vas: Vascular (e.g., CTVvas)
3/ When different target areas appear, add classification symbols at the end of the target area (e.g., PTV1, PTV2, GTVp1, GTVp2);
4/ For adaptive radiation therapy, when imaging modalities and sequences need to be recorded, follow the type/classification symbol/ enumeration style before the underscore, and then supplement with the imaging modality (CT, PT, MR, SP) and the number of images used in the sequence (e.g., PTVp1_CT1PT1, GTV_CT2);
5/ When using structural indicators, follow the type/classification symbol/enumeration style before the underscore and use its number to represent the reviewed structure naming list (e.g., CTV_A_Arota, CTV_A_Celiac GTV_Preop, PTV_Boost, PTV_Eval, PTV_MR2_Prostate);
6/ When indicating dose, the dose is placed at the end of the target area string with an underscore character. The working group strongly recommends using relative dose levels rather than absolute doses to specify physical doses;
High (PTV_High, CTV_High, GTV_High)
Low (PTV_Low, CTV_Low, GTV_Low)
Mid (PTV_Mid, CTV_Mid, GTV_Mid)
7/ If it is necessary to indicate the numerical value of physical dose, it is strongly recommended that these values must be in cGy (e.g., PTV_5040);
8/ If it is necessary to use numerical values of physical dose, these values must be in Gy, and Gy should be added to the dose value (e.g., PTV_50.4Gy). If this form is not allowed by the system, replace the decimal point with “p” (e.g., PTV_5050p4Gy);
9/ The dose must reflect the number of treatments required to achieve the total dose requirement, and the dose/treatment values must be expressed in cGy or Gy and followed by the dose unit. Additionally, use “x” to separate the number of treatments and dose/treatment, with the number of treatments appended after “x” (e.g., PTV_Liver_2000x3 or PTV_Liver_20Gyx3);
10/ When it is necessary to include the patient’s contour, place “-xx mm” at the end of the target area string. Its length follows the dose representation method and is expressed in xx mm style (e.g., PTV_Eval_7000-08, PTV-03, CTVp2-05);
11/ When using custom strings, they need to be appended after “^” (e.g., PTV^Physician1, GTV_Liver^ICG)
12/ If it is not possible to follow the above guidelines and maintain the 16-character limit, retain the relative order but require the removal of underscores, implementing this from left to right until the limit condition is met (e.g., PTVLiverR_2000x3);
2. Non-target Structure Naming Suggestions
1/ To be compatible with most VADE systems, all structure names are limited to 16 characters or less;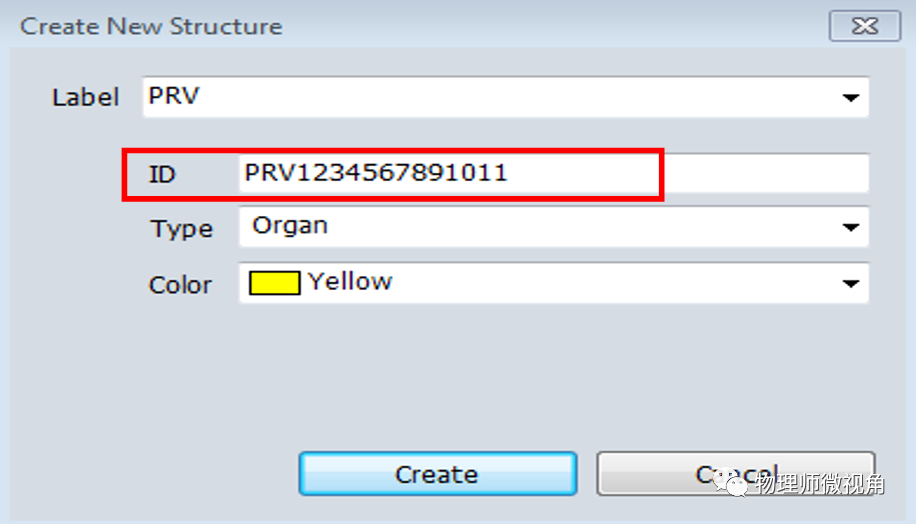
2) Use underscores to separate categories (e.g., Bower_Bag)
3) Characters representing spatial categories are placed at the end of the main name, separated by underscores (e.g., Lung_L, Lung_LUL, Lung_RLL, OpticNrv_PRV03_L)
L represents left side
R represents right side
A represents anterior side
P represents posterior side
I represents inferior side
S represents superior side
V represents vein (e.g., V_Portal, V_Pulmonary)
LN represents lymph node (e.g., LN_Ax_L1, LN_IMN)
CN represents cranial nerve (e.g., CN_IX_L, CN_XII_R)
Glnd represents gland (e.g., Glnd_Submand)
Bone represents bone (e.g., Bone_Hyoid, Bone_Pelvic)
Musc represents muscle (e.g., Musc_Masseter, Musc_Sclmast_L)
Spc represents space (e.g., Spc_Bowel, Spc_Retrophar_L)
VB represents vertebra
Sinus represents sinus (e.g., Sinus_Frontal, Sinus_Maxillary)
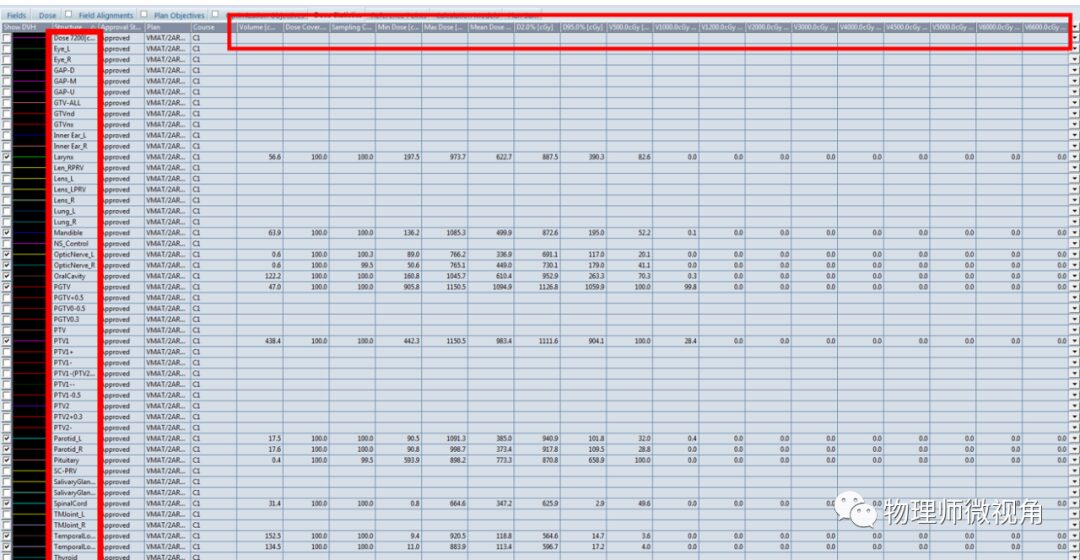
3. Recommendations for Dose-Volume Histogram Standards
Input accurate parameters, dose, and volume units; all formats are parsed with regular expression operators to enhance the ability of computer algorithms to automatically calculate.

Reviewed by: Wang Lu Proofread by: Luo Ying Yang Siyao Editor: Guo Zhiwei Organized by: Jiang Shewei
[Statement] This public account aims to disseminate more information, and the copyright of the interpreted article belongs to the original author. The content reflects the views of the original author, and this public account is not responsible for its authenticity, nor does it constitute any clinical application advice. If there are issues regarding the content, copyright, and other matters, please contact this public account within 30 days, and we will delete the content at the first opportunity! This public account reserves the right of final interpretation of this statement!
Scan the QR code for more surprises
