As drug development becomes increasingly globalized, Multi-Regional Clinical Trials (MRCT) have become an important tool for supporting the simultaneous approval of drugs worldwide. The ICH E17 guidelines, released in November 2017 by the International Council for Harmonisation (ICH), provide a systematic framework for the planning and design of MRCTs. This article aims to provide a professional interpretation of the core content of these guidelines, helping researchers and regulatory agencies better understand and apply this guidance.
Background and Purpose
The background for the development of ICH E17 stems from the challenges posed by the globalization of drug development. Different regulatory agencies may have varying, and even conflicting, requirements for clinical trials, which increases the complexity of global drug development. The goal of E17 is to enhance the acceptability of MRCT designs in global regulatory submissions by standardizing their design principles, thereby accelerating the process of bringing new drugs to market worldwide.
E17 applies to clinical trials conducted in multiple regions under a single protocol, with data used to support drug approvals (including new indications, new formulations, or new administration routes) or to meet post-marketing study requirements. This guidance emphasizes the synergistic use of other ICH guidelines (such as E5, E6, E8, E9, E10, and E18).
Basic Principles of MRCT
E17 outlines seven basic principles for MRCT design, which include:
-
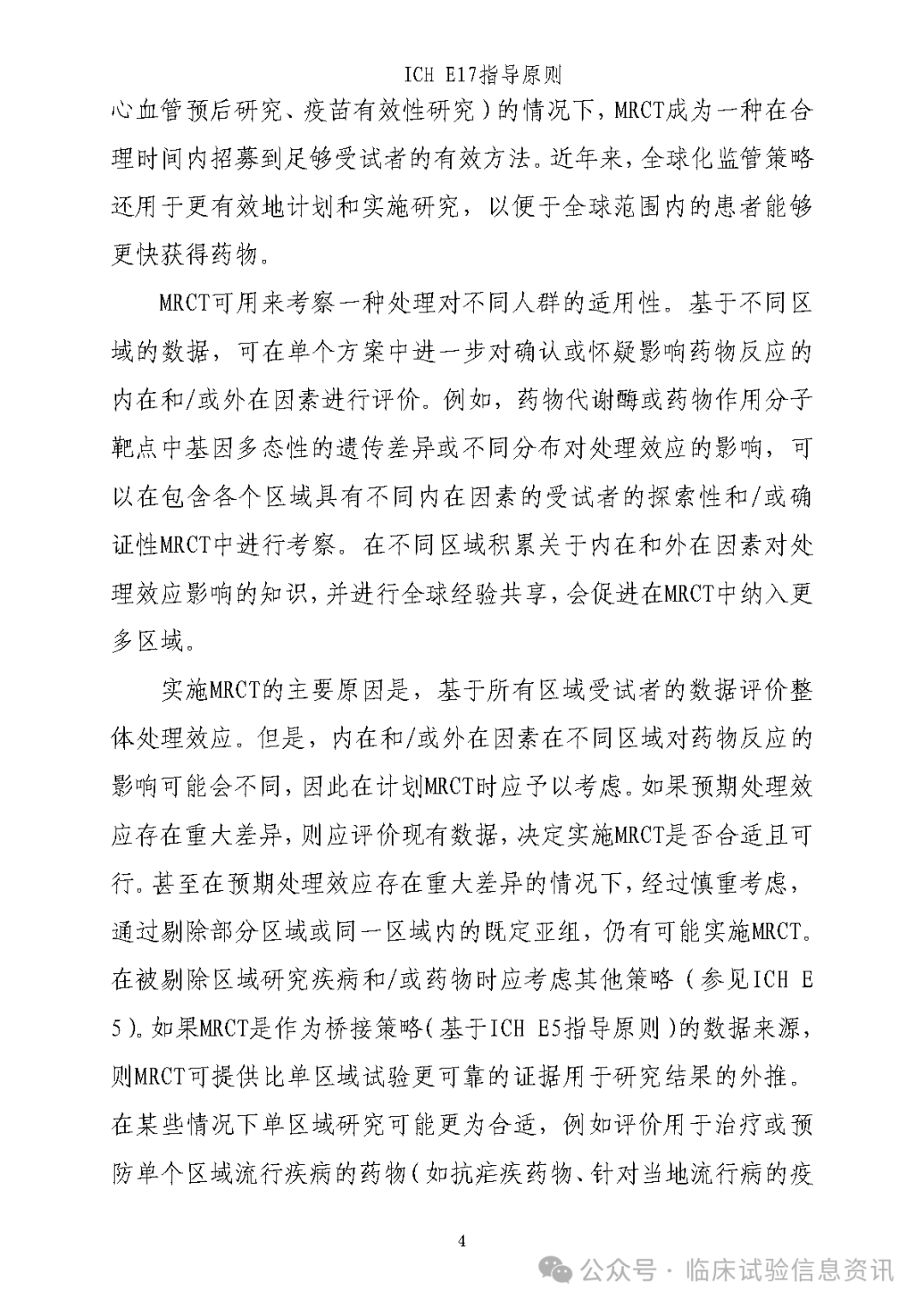
Strategic Use of MRCT: By designing and executing MRCTs effectively, development efficiency can be improved, supporting simultaneous submissions for marketing applications across multiple regions.
-
Early Identification of Influencing Factors: Investigate intrinsic and extrinsic factors (such as ethnicity and medical practices) that may potentially affect drug responses during the exploratory phase.
-
Assumptions of Treatment Effect Applicability: MRCT designs are based on the assumption that treatment effects are applicable to the entire target population, which must be validated through regional sample size allocation.
-
Merging Regions or Subgroups: Pre-merge regions or subgroups based on similarities to support the evaluation of treatment effect consistency.
-
Analytical Methods: The primary analytical methods must be accepted by all relevant regulatory agencies while structurally exploring the consistency of treatment effects across regions.
-
High-Quality Implementation: Ensure research quality by strictly adhering to ICH E6 (GCP) requirements.
-
Regulatory Communication: Encourage scientific consultation with regulatory agencies during the MRCT planning phase.
Key Recommendations for MRCT Planning and Design
1. Strategic Issues
-
Value of MRCT: MRCTs can efficiently recruit subjects, especially suitable for studies involving rare diseases or large populations. Additionally, they support the evaluation of drug responses across different populations, facilitating simultaneous global drug development.
-
GCP Requirements: All research centers must comply with ICH E6 GCP standards to ensure trial quality and data reliability.
-
Regulatory Consultation: It is recommended to communicate with regulatory agencies during the MRCT planning phase to ensure that the study design meets multi-regional regulatory requirements.
2. Trial Design and Protocol Issues
-
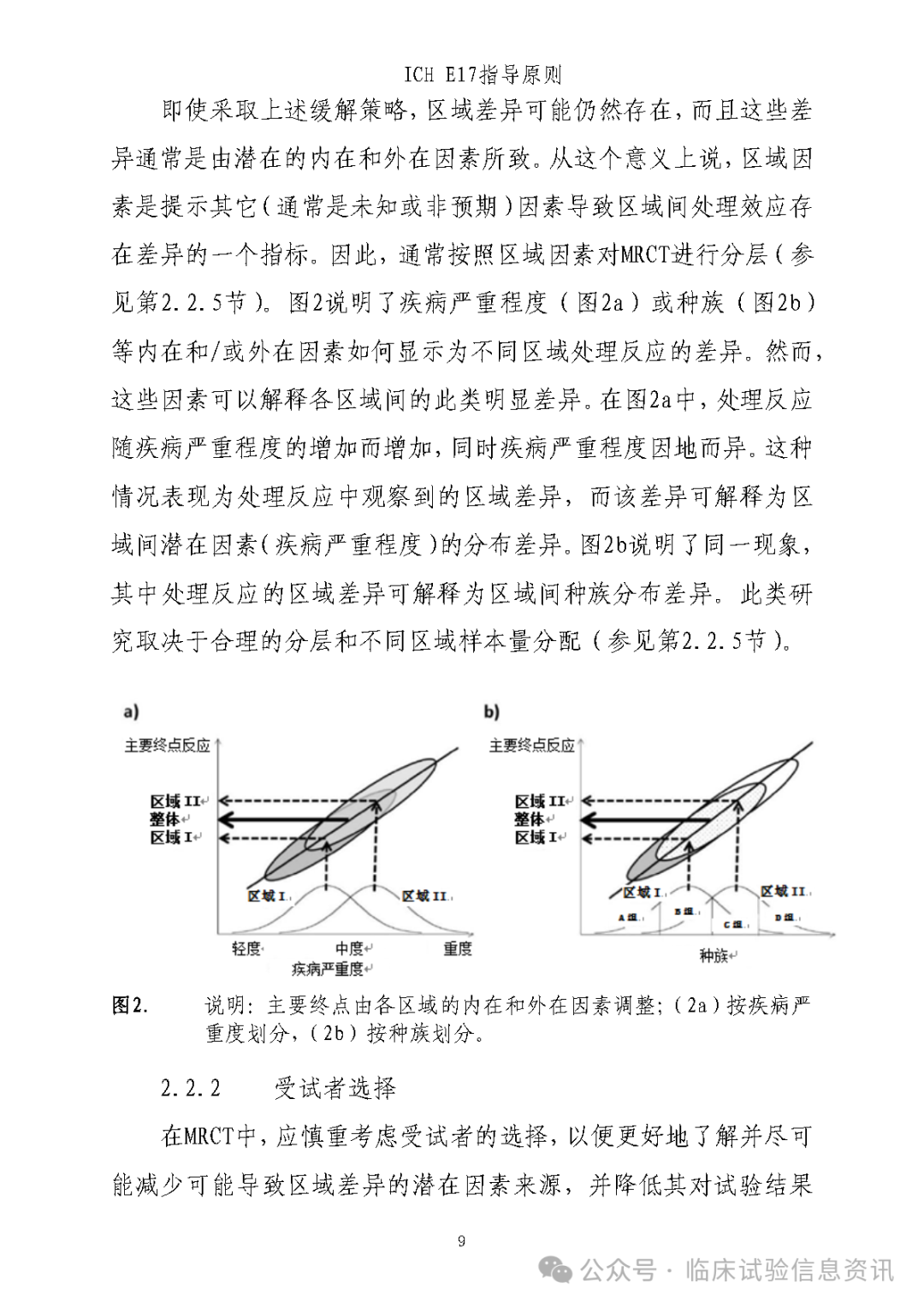
Pre-Consideration of Regional Differences: Identify potential regional differences that may affect efficacy and safety, such as disease definitions, medical practices, and cultural factors, and reduce the impact of these differences through standardized protocols and training.
-
Subject Selection: Standardize inclusion and exclusion criteria, using internationally recognized diagnostic tools and scales to ensure regional consistency in subject selection.
-
Dosing Selection: Early PK/PD studies should cover the target regional population, and dosing selection should be based on scientific evidence, with discussions with regulatory agencies as necessary.
-
Endpoint Selection: Primary endpoints must be accepted by all relevant regulatory agencies and have clinical relevance. Secondary endpoints should be as uniform as possible to avoid multiplicity adjustment issues.
-
Sample Size Planning: The total sample size must ensure the evaluation of overall treatment effects; regional sample size allocation should be scientifically reasonable to avoid results being dominated by a single region. Merging regions or subgroups can enhance flexibility.
-
Statistical Analysis: Primary analyses should adjust for regional stratification and structurally explore the consistency of treatment effects. Interaction tests may have low power and should be interpreted in conjunction with clinical rationale.
-
Control Selection: In principle, all regions should use the same control; if there are differences between regions, scientific justification and documentation are required.
-
Concomitant Medications: Standardize concomitant medications as much as possible, and document and assess the impact of regional differences on results.
-
Management of Regional Differences: Reduce implementation differences through standardized training, centralized monitoring, and electronic data collection.
-
Sample Size Allocation: Balance scientific rigor with operational feasibility to avoid unreliable results due to insufficient regional sample sizes.
-
Regulatory Coordination: Different regulatory agencies may have conflicting requirements, necessitating early communication to reach consensus.
Conclusion: ICH E17 provides comprehensive guidance for the design and implementation of MRCTs, with the core focus on ensuring that MRCTs can support multi-regional regulatory decisions through scientifically sound planning, thereby accelerating the global market entry of new drugs. In the future, as drug development continues to globalize, the application of E17 will become more widespread, while also requiring ongoing optimization and innovation to address new scientific and regulatory challenges.
For sponsors, adhering to the principles of E17 not only enhances development efficiency but also increases regulatory agencies’ trust in MRCT data, potentially providing patients with earlier access to innovative treatments.