Background
In the Russia-Ukraine war, the use of high-energy weapons such as shells, cruise missiles, drones, and expanding bullets has resulted in numerous severe soft tissue injuries, as well as segmental bone defects or significant bone loss.
During the local conflicts from 2014 to 2022, upper limb injuries were quite frequent. Among these, humeral fractures accounted for as much as 9.5%, and the rate of shoulder amputations among combat casualties reached 0.5%. Research data indicates that the incidence of purulent complications among Ukrainian casualties ranged from 21.4% to 25.6%, while the incidence of gunshot-related osteomyelitis was between 12% and 14%. These complications often prolong the patients’ hospital stay and adversely affect the recovery of anatomical structure and functional outcomes, leading to less than ideal treatment results.
For the management of gunshot fractures, an important task is to correctly reposition bone fragments and achieve stable fixation to expedite the patient’s recovery process. To optimize preoperative planning, three-dimensional (3D) printing technology, also known as additive manufacturing, has been actively applied in routine orthopedic practice. As early as the early 1990s, 3D printing technology was introduced into the orthopedic field, where it was used to create single templates with insertion screw guides for knee replacement surgeries.
Today, preoperative 3D printing technology also holds application value in military orthopedics and trauma surgery, bringing improvements in several aspects: first, it aids in reasonable preoperative planning and intraoperative localization; second, it can be used to produce individual metal fasteners (such as titanium 3D printed products); third, it can design individual implants and meshes (containers) made from plastic materials and biodegradable materials; fourth, it can create tools for performing complex surgical operations.
Exploring new 3D printing methods and applying existing 3D printing techniques may improve the treatment of severe gunshot wounds (including large bone defects). Given the severity of gunshot injuries in the Russia-Ukraine war, it is necessary to improve treatment strategies, especially in the management of large bone defects.
A series of previously published articles have confirmed that various methods have certain efficacy in the treatment of gunshot wounds, such as using bone biological materials, performing closed reduction, applying percutaneous lag screws for significant compression, utilizing Ilizarov external fixation (i.e., double local osteosynthesis), and employing 3D printing technology. It is noteworthy that gunshot wounds have been thoroughly studied in various wars and armed conflicts, including research related to the mixed period of the Russia-Ukraine war from 2014 to 2020 and beyond.
However, since the outbreak of the Russia-Ukraine war on February 24, 2022, research on the current status of orthopedic trauma treatment and the potential role of 3D printed PEEK implants has been relatively scarce. In this study, we hypothesize that 3D printed PEEK implants can be used to treat severe humeral fractures associated with high-energy weapons.
This study aims to evaluate various treatment methods for combat casualties with severe humeral defects and share the experiences of orthopedic war surgeons in managing humeral gunshot wounds during the current war.
Patients and Methods
This study selected 24 subjects, all of whom were active-duty soldiers of the Ukrainian Armed Forces injured on various battlefields in Ukraine. The non-confidential data for the study were collected from February 24, 2022, to January 1, 2023.
The inclusion criteria for the study were confirmed humeral shaft gunshot fractures, while exclusion criteria included the occurrence of osteomyelitis after gunshot wounds, severe microbial contamination of the wound (colony-forming units (CFU) > 10⁶/ml), and complete transection of the radial and ulnar nerves. The causes of injury for these casualties were various high-energy weapons, such as self-propelled multiple rocket launcher systems, artillery, mortar shelling, cruise missile attacks, and drone (unmanned aerial vehicle) strikes.
The study employed the 2018 revised AO/OTA classification of fractures and dislocations to determine the complexity of the fractures. All patients underwent routine clinical chemistry tests and urinalysis after admission to a level IV military hospital. Additionally, X-ray imaging was performed with two projections, and computed tomography (CT) scans were conducted on the injured limbs, along with Doppler imaging of the vessels to clarify the characteristics of the main and collateral blood supply to the injured upper limb, and CT angiography was used to identify the vascularized bone fragments.
Upon admission, patients were assessed for comorbidities, wound and skeletal structural changes, the degree of inflammatory changes in the area of removed pins, and potential damage to the major vessels in all patients, including possible ischemia and venous thrombosis in the injured limb segment. Furthermore, the degree of microbial contamination was determined by calculating the CFU for all patients, and microbiological examinations of the wounds were conducted.
The treatment process for patients was divided into three stages, each aimed at addressing specific issues in wound management. This article focuses on the second stage, with a brief overview of each stage as follows:
- Stage I: All casualties underwent damage control surgery, secondary check surgeries, reconstructive surgeries, primary surgical debridement, fasciotomy, focal external fixation, and antibacterial joint spacers treatment. Additionally, VAC machines (vacuum-assisted closure systems) KCI (HEACO, China) and Sonoca 185 (Söring, Germany) were used for ultrasonic cavitation and vacuum-assisted closure (VAC) treatment as previously described.
- Stage IIA: This stage primarily involved the replacement (conversion) of orthopedic fixation devices. To achieve the conversion from external fixation, 3D imaging technology was used preoperatively to accurately determine the position, size, and shape of the humeral fragments, thereby constructing a virtual repair model of the humerus. 3D imaging also aided in selecting or developing the components needed for fixation, determining whether grafts were needed to replace parts of the bone to restore its shape, and clearly presenting the location of blood vessels to minimize the risk of intraoperative vascular injury. The first step in creating a physical 3D model was processing two-dimensional CT images, with orthopedic surgeons analyzing each CT slice to remove all artifacts. Subsequently, the CT images were converted from DICOM format to STL format using Mimics Medical 24.0 software for subsequent 3D printing; Graphics Medical 14.1 software was used to rotate the 3D model in all dimensions and connect it with other components, such as using a blocked intramedullary rod or a Philos plate suitable for proximal third humeral fractures.
- Stage IIB: This stage involved reconstructive and restorative surgical interventions, including the replacement of bone defects. Polyether ether ketone (PEEK) was used as a bone biological material to replace the bone defects, with 3D printing based on PEEK. Additionally, the replacement of bone defects could also be completed through closed reduction, significant compression using percutaneous lag screws, and Ilizarov external fixation, while vascularized fibula was also used as a graft to replace the bone defect.
- Stage III: All patients received treatment at rehabilitation centers in Ukraine and abroad; this study did not obtain data on physical rehabilitation management during this stage.
The study followed up with patients at 3 months, 6 months, and 12 months. During follow-up, parameters such as the time from injury to reconstructive surgery, duration of surgical intervention, range of motion (ROM) of the shoulder and elbow joints, neurological status and improvement, and the occurrence of complications (such as osteomyelitis, heterotopic ossification, instability of orthopedic implants, failure of bone consolidation, formation of pseudoarthrosis, and autologous bone loosening) were assessed. Additionally, the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire was used to evaluate the upper limb disability status and related symptoms of patients 12 months post-injury.
This study was approved by the Ethics Committee of Bogomolets National Medical University (Kyiv, Ukraine). Due to the ongoing conflict, the government has kept detailed clinical information about the casualties confidential. Given the small sample size of the cohort, this study is not suitable for statistical analysis and is classified as a “descriptive study.”
Conclusion
All patients sustained severe injuries due to shelling, and all were male, with an average age of 33.8 years. The average time from injury to admission to a level IV hospital for treatment was 1.6 days.
According to the 2018 revised AO/OTA classification of fractures and dislocations, 4 patients (17%) had simple type A fractures, 8 patients (33%) had type B fractures, and 12 patients (50%) had segmental and comminuted type C fractures. The characteristics of the comminuted severe fractures of the humerus can be referenced in Figures 1 and 2.
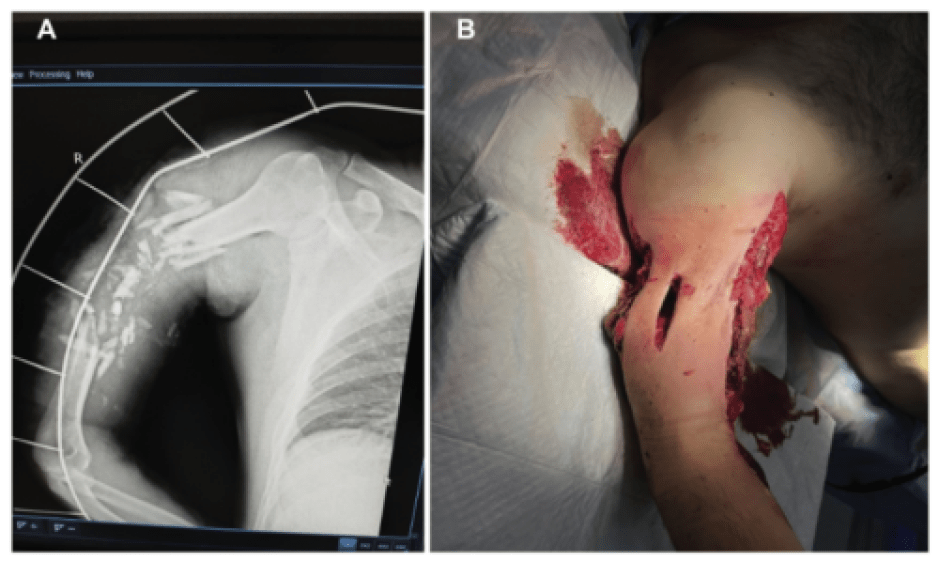
Figure 1. Photos of a patient with multiple fractures of the right humerus, showing bone loss and fragment displacement. A. X-ray showing severe fracture; B. Preoperative photo
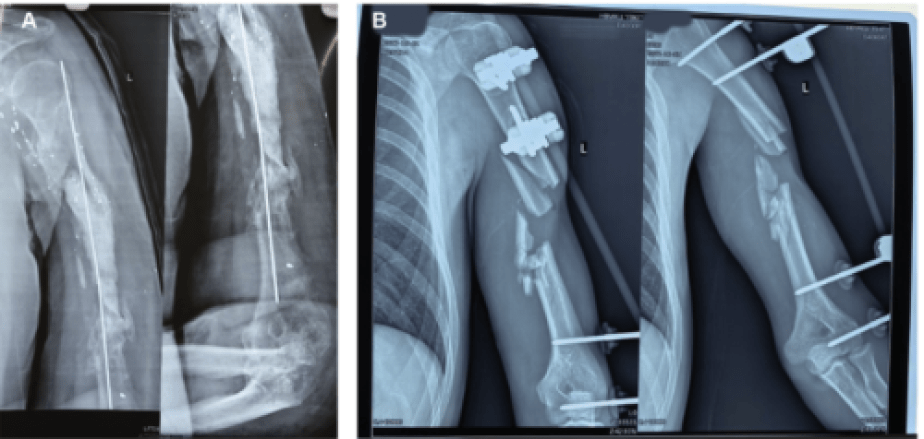
Figure 2. X-ray film of a gunshot fracture of the left humerus. A patient with multiple fractures of the left humeral shaft, showing bone loss and fragment displacement. B. Gunshot comminuted fracture at the mid-shaft of the left humerus, with bone loss and fragment displacement.
Analysis of the microbial contamination of wounds upon patient admission indicated an average colony-forming unit (CFU) value of 10/ml, ranging from 10-10/ml. Within 21-24 days from baseline, the degree of microbial contamination decreased in 21 patients (88%), with the average CFU value dropping to 10/ml, ranging from 10-10/ml.
Among the 24 patients, 3 (13%) were diagnosed with segmental bone loss of 5 cm in the humerus, 4 (17%) patients also had segmental bone loss of 5 cm, and 17 (71%) patients had defects of 10 cm or more. Among these 17 patients (71%), 5 received treatment with 3D printed PEEK implants (details can be seen in Figures 3, 4, 5), 6 were treated with closed reduction, percutaneous lag screws combined with Ilizarov external fixation, and another 6 underwent vascularized fibula grafting (details can be seen in Figure 6).
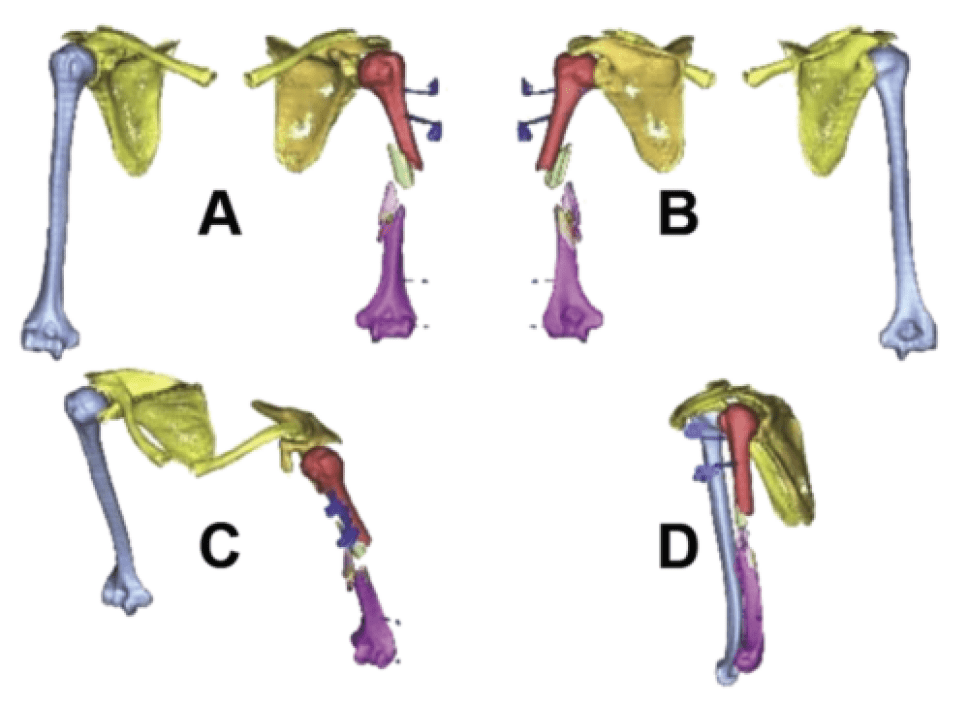
Figure 3: 3D modeling explanation: Processing two-dimensional CT images of a patient with multiple fractures of the left humeral shaft, showing fragment displacement.

Figure 4: Illustration of the 3D modeling stage. A. Comparison of bone fragments to assess the possibility of restoring the integrity of the damaged bone structure in patients with multiple fractures of the right humeral shaft, showing fragment displacement; B. Illustration of the final stage of 3D modeling of PEEK material.
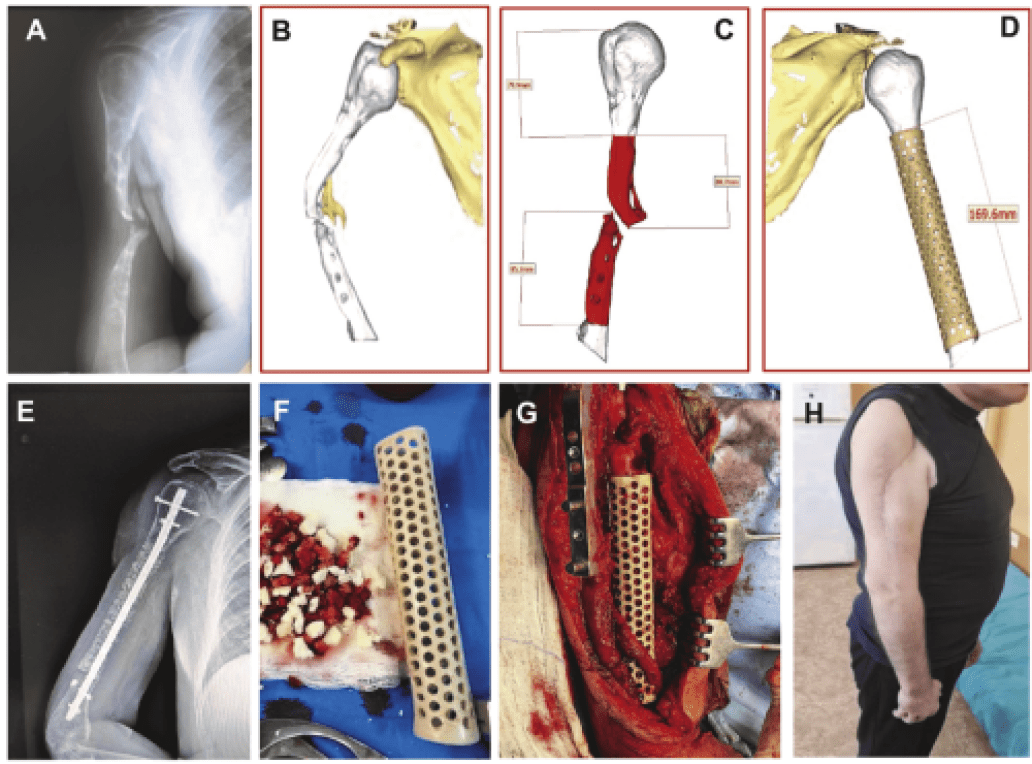
Figure 5: Photos of a patient with severe fractures of the right humerus treated with 3D printed PEEK implants.
|
Notes: A. Preoperative X-ray showing severe bone loss >10cm, with pseudoarthrosis at the mid-third of the humerus, and defects in the bone structure, with sclerotic lesions at both proximal and distal ends. B. Preoperative 3D modeling graphics determined the formation of pseudoarthrosis and changes in the bone axis. C. Preoperative 3D modeling illustrating the size calculations for further resection of the sclerotic portions of the proximal (69.7mm) and distal (85.2mm) humerus. D. Schematic diagram of the 3D modeling of the PEEK implant before surgery. E. Postoperative X-ray at 12 months showing that the bone defect was replaced by cortical cancellous granules, with signs of consolidation in the right humerus, fixed with closed nails. F&G. Intraoperative photos of the 3D printed PEEK scaffold, with combined allogenic materials placed on the scaffold for humeral shaft defects. H. Photos of the patient’s right upper limb showing postoperative scars at 12 months. |
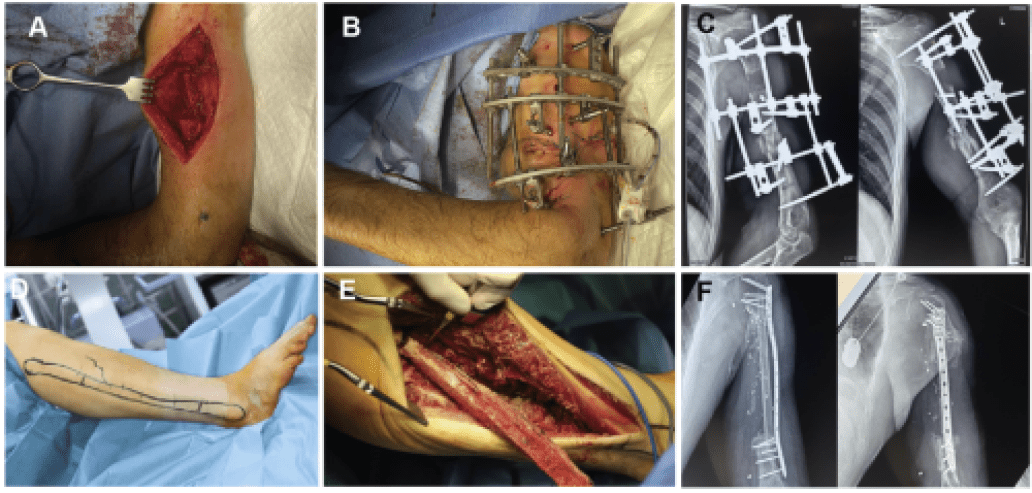
Figure 6: Clinical photos of the patient showing the treatment stages of closed reduction, percutaneous lag screws, and Ilizarov external fixation (A, B, C) as well as vascularized fibula grafting (D, E, F).
Patients treated with 3D printed PEEK implants had an average follow-up time of 14.8 months. Among these patients, the average time from injury to reconstructive surgery was 5.3 months, and the average duration of surgery was 80.4 minutes. The average DASH score at baseline was 75.3, which improved to 49.6 at the 12-month follow-up, indicating self-reported improvement. X-ray analysis showed no signs of heterotopic ossification. CT scans at 12 months post-injury revealed that bone bridges formed between the autologous allogenic materials within the PEEK lattice and the main fragments. After using PEEK implants, one case (20%) was diagnosed with osteomyelitis, requiring the removal of the PEEK implant and metal implants, followed by the application of antibiotic spacers and humeral ExFix fragments. We believe that the occurrence of osteomyelitis was due to insufficient wound debridement and non-compliance with conversion standards (replacement of fixation methods). The average hospital stay for patients treated with 3D printed PEEK implants was 5.5 months.
Six patients treated with closed reduction, percutaneous lag screws, and Ilizarov external fixation had a follow-up of 13.4 months. Among these patients, the average time from injury to reconstructive surgery was 5.8 months, and the average duration of surgery was 78.1 minutes. The average DASH score at baseline was 73.1, which improved to 33.4 at the 12-month follow-up, indicating self-reported improvement. In one patient, heterotopic ossification and the development of paravertebral osteomyelitis were observed, necessitating the removal and placement of a viewing rod. The average hospital stay for this group of patients was 3.5 months.
Six patients who underwent vascularized fibula grafting had a follow-up of 14.1 months. Among these patients, the average time from injury to reconstructive surgery was 5.5 months, and the average duration of surgery was 112 minutes. At the 12-month follow-up, the average DASH scores were 74.3 and 32.7, indicating self-reported improvement. Two patients were diagnosed with heterotopic ossification. The average hospital stay for this group of patients was 6.5 months.
Overall, 4 patients (17%) were diagnosed with postoperative complications. Among the 17 patients with segmental humeral defects, complication analysis revealed >2 patients with seromas, which were managed through wound drainage and VAC treatment.
Among the 6 patients treated with closed reduction, percutaneous lag screws, and Ilizarov external fixation, 2 had issues with the rods, requiring appropriate care for the external fixation devices, while the other 4 patients underwent double local osteosynthesis without postoperative complications. In 2 patients who underwent vascularized fibula grafting, serous hemorrhagic exudates were diagnosed, which were treated with VAC therapy. No complications were observed in the other 4 patients who underwent vascularized fibula grafting.
Discussion
This study confirms that modern technologies such as 3D printing of PEEK implants can be applied in level III and IV care settings (including field hospitals and rear hospitals). This study is the first to demonstrate the specific characteristics of combat-related upper limb injuries and to share experiences in managing long bone (i.e., humeral) fractures using 3D modeling with PEEK. 3D printed PEEK implants are frequently used in maxillofacial surgeries and civilian orthopedic surgeries, but rarely for war-related injuries.
The findings of this study confirm that modern technologies such as 3D printing with PEEK implants represent a potential method for treating severe defects in long bones. The results are consistent with those of Hamsho et al., indicating the practicality of PEEK implants in reconstructing maxillary defects caused by sniper gunshot wounds in a war environment. However, the application of these technologies faces challenges due to disruptions in medical supplies and overall issues within the Ukrainian healthcare system. The choice to use PEEK instead of other implants is due to its superior bone integration and antibacterial properties. It is worth noting that 3D printing and PEEK implants are primarily used for reconstructing maxillofacial deformities related to gunshot wounds or brain tumors, but this technology has not previously been applied to reconstruct long bones such as the humerus in combat patients. Despite the relatively high incidence of complications found (1 in 5 injured), the study indicates that 3D printing and PEEK implants can be used to treat long bone defects following high-energy weapon gunshot wounds, consistent with findings by Hamsho et al. and Chaiyasat et al. showing the practicality of PEEK for maxillofacial PEEK implant reconstruction and cranioplasty patients.
Due to the inherent biological inertia of PEEK, the potential limitations of its widespread use for bone defect repair should be considered, as this may lead to fibrotic changes around the implant, negatively impacting bone integration. However, in the case of severe defects in long bones related to warfare, the utility of PEEK implants is considered to outweigh the potential risks of impaired bone integration. The study also found a relatively low frequency of wound infection among postoperative complications, indicating that the management plan for late-stage treatment was appropriate.
Considering the mechanical properties of PEEK being similar to those of human bone tissue and its high radiolucency, the use of 3D printed PEEK implants for bone reconstruction shows promise for combat-related long bone injuries. However, the fibula serves as a good graft for reconstructing long bone defects. Heitmann et al. demonstrated overall utility in using fibula grafts in 15 patients with segmental humeral defects, yielding good results, although the incidence of postoperative complications was high. Vascularized fibula grafting is associated with good outcomes, as the grafted bone integrates better with the recipient bone, reducing the risk of pseudoarthrosis and graft fractures, as well as minimizing hypertrophic changes of the fibula graft under physiological axial loading. The study also demonstrated a relatively low incidence of postoperative complications among injured patients, indicating that fibula grafting is a good method for selected patients’ bone reconstruction. Ilizarov distraction osteogenesis is commonly used for fractures related to civil wars and warfare. This method is well-suited for use in conjunction with closed reduction and percutaneous lag screws for treating severe bone defects, as it is associated with sufficient bone compression. However, the Ilizarov method is not suitable for fixing smaller bone fragments commonly seen in battlefield trauma.
Original link: https://www.sciencedirect.com/science/article/pii/S002013832300997X
(Source: Yisi Space. Copyright belongs to the original author. If there is any infringement, please contact for deletion.)