
This article defines the current community embedded elderly care as “a new type of elderly care model that integrates various service resources through sinking and integration to create a comprehensive elderly care complex within the community, allowing elderly individuals to enjoy quality care services close to home.”
It should be noted that although community embedded elderly care contains the word “community,” it cannot be directly equated with traditional community elderly care or community home-based elderly care. In community embedded elderly care, the “community” serves dual meanings as both the provider of elderly care services and the location for using these services, thus representing a collection of quality content from community elderly care and community home-based elderly care.
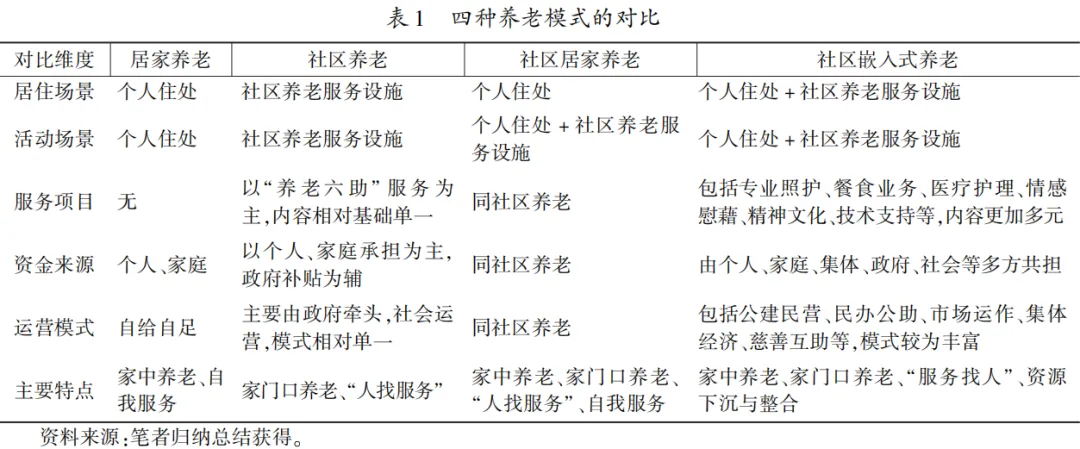
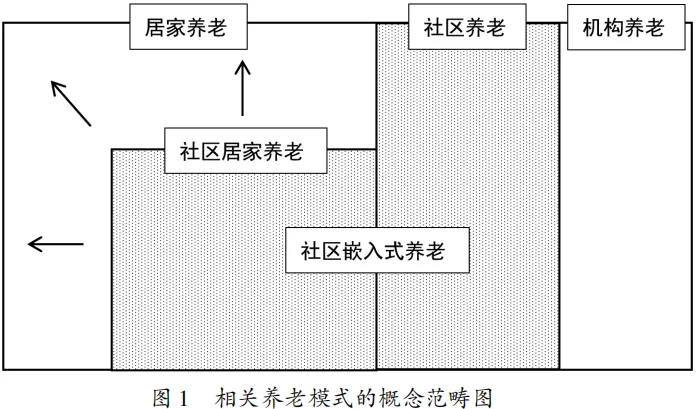
To further differentiate the similarities and differences among various elderly care models, this article compares home-based elderly care, community elderly care, community home-based elderly care, and community embedded elderly care from dimensions such as living scenarios, activity scenarios, and service projects, accompanied by a conceptual category chart of elderly care models, as detailed in Table 1 and Figure 1.
Current Development Status of Community Embedded Elderly Care in China
Based on the aforementioned analytical framework, this article focuses on the dimensions of demand embedding, resource embedding, subject embedding, and concept embedding in community embedded elderly care, systematically sorting out the service projects, service facilities, and operational models within community embedded elderly care, aiming to better present the overall development of community embedded elderly care in China.
1. Service Projects of Community Embedded Elderly Care
The service projects of community embedded elderly care are quite broad. Currently, domestic scholars are generally more focused on the care and nursing attributes of community embedded elderly care in relevant studies, but in fact, the service projects of community embedded elderly care go far beyond this.
Based on the review of relevant policy documents released by some leading regions and recent research findings, this article roughly categorizes the service projects of community embedded elderly care into professional care, meal services, medical care, emotional comfort, cultural and spiritual services, technical support, and other services, with each category further including different service projects, as detailed in Table 3.
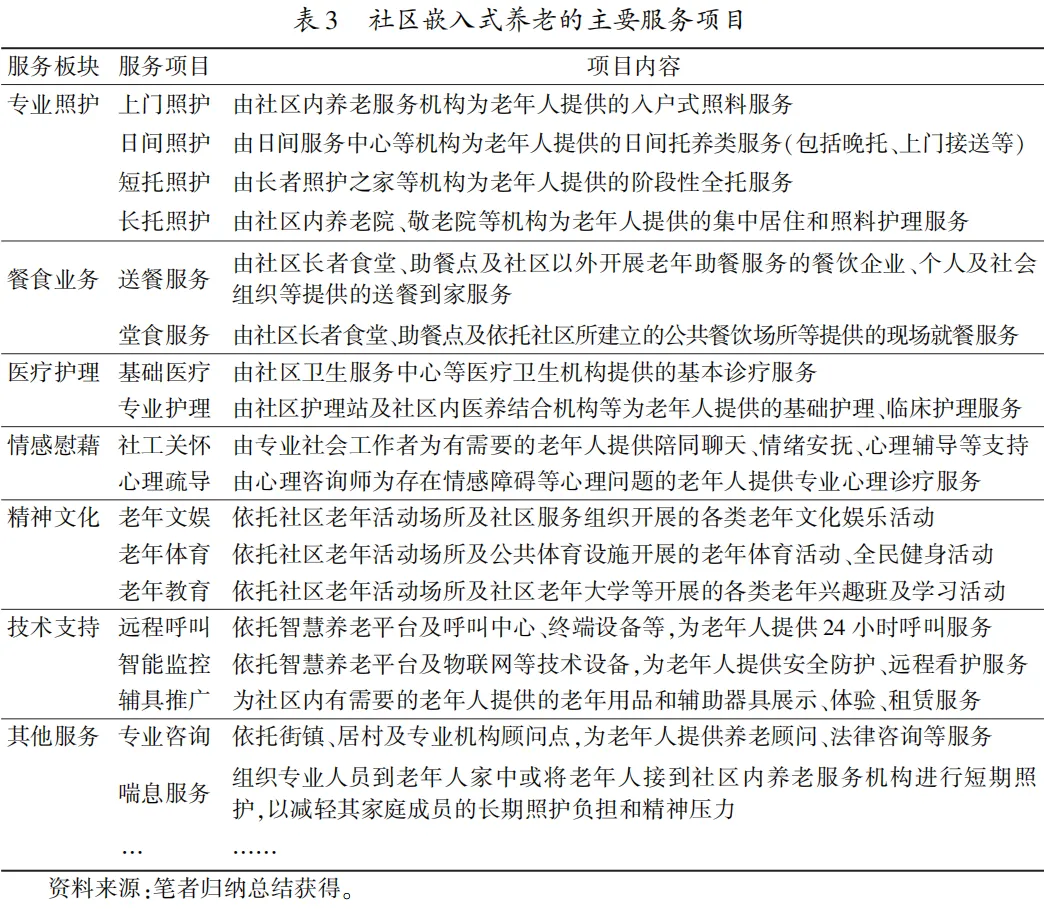
First, the professional care sector is the core of community embedded elderly care.This type of service focuses on addressing the questions of “where to care,” “who will care,” and “how to care” in traditional elderly care models. Since the service projects in this sector (especially daytime care and short-term care) possess strong integration and nesting properties, some scholars have equated this type of service directly with community embedded elderly care. However, as the connotations of related services have enriched and the forms of embedding have diversified, the relationship between the two has been further clarified.
Second, meal services and medical care are the foundational components of community embedded elderly care.These services primarily meet the two major needs of elderly individuals in the community for food and medical care, corresponding to the most basic physiological and safety needs in Maslow’s hierarchy of needs. Therefore, the total demand for related services is large and urgent; meal services and medical care have become key supporting sectors in the construction of community embedded elderly care services.
Third, emotional comfort, cultural and spiritual services, technical support, and other services are important supplements to community embedded elderly care.These services can better meet the multi-layered and personalized material and spiritual needs of elderly individuals in the community, improving their quality of life, corresponding to the higher-level needs of social interaction, respect, and self-actualization in Maslow’s hierarchy. However, due to differences in the foundational conditions and development levels among different regions, the promotion of service projects in these sectors is generally lower, and the development gap among different regions is relatively larger.
2. Service Facilities of Community Embedded Elderly Care
Home-based, community, and institutional facilities are important spatial carriers for the sinking of socialized elderly care service resources to the grassroots. Based on the placement locations, functional positioning, and service cycles of different service facilities, this article specifically divides the service facilities of community embedded elderly care into three categories: home-based, community daytime, and institutional residential facilities, with details of the classifications and the primary service facilities corresponding to each type presented in Figure 2.
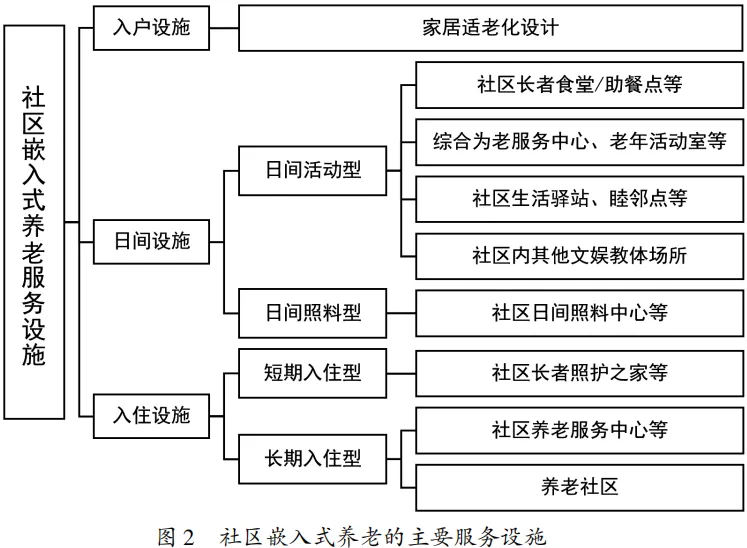
First, home-based facilities.These primarily target elderly individuals who are long-term home dwellers, with representative facilities being various types of home adaptations for the elderly, such as safety handrails, non-slip floors, indoor sensor lights, elderly seating and bedding, smart home devices for the elderly, and monitoring call systems. These adaptations can effectively reduce the difficulty of elderly individuals’ home activities, and some smart devices even have networked functions for risk alerts and emergency assistance. Multi-form, multi-scenario, and multi-functional home facilities work together to create a safe, convenient, and comfortable home-based elderly care environment.
Second, community daytime facilities.These include daytime activity and daytime care types. The former primarily targets elderly individuals with intact mobility and relatively good health. From the perspective of functional integration, these facilities can be further divided into single-type (e.g., community senior dining halls) and compound-type (e.g., comprehensive elderly service centers, community life stations). Related facilities widely cover a series of functions including dining, social interaction, entertainment, sports, and education, which can effectively meet the multi-layered elderly care needs of individuals in the community, improving their quality of life. The latter is represented by community daytime care centers that provide day care services.
Third, institutional residential facilities.These include short-term and long-term residential types. The former is represented by community elder care homes, which provide full-time care services for elderly individuals and families in need (e.g., when no one is available to care for them at home or when short-term rehabilitation is required due to illness). To allow more elderly individuals in the community to receive care, short-term residential facilities usually impose limits on the duration of stay. The latter is represented by community elderly service centers and other institutions. Additionally, some scholars have also categorized the gradually emerging elderly care communities in recent years into this type of facility.
3. Operational Models of Community Embedded Elderly Care
Currently, domestic scholars mainly classify the operational models of community embedded elderly care from two perspectives: one is based on the overall characteristics of geographical regions, such as the Shanghai model, Beijing model, Chongqing model, Hefei model, and Shijiazhuang model; the other is based on specific service performance forms, such as the “Party Building + Elderly Care” model, “Property Management + Elderly Care” model, and elderly care station model.
Similar to traditional institutional elderly care, the development of community embedded elderly care relies on the government but also requires extensive participation from social entities. Different entities perform their respective roles and embed with each other, resulting in a rich variety of operational models. Based on this, this article summarizes five main operational models of community embedded elderly care, including public construction and private operation, private funding and assistance, etc., as detailed in Table 4.
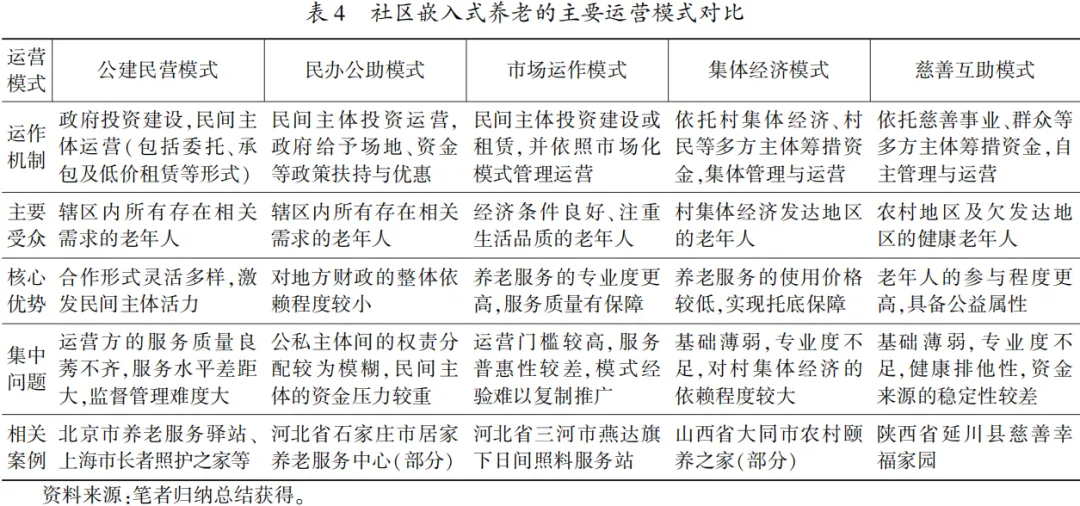
Overall, the five operational models of community embedded elderly care currently exhibit distinct characteristics, each with its strengths and weaknesses. Among them, the public construction and private operation model has the highest prevalence nationwide and holds an absolute position in economically developed provinces and cities such as Beijing and Shanghai. This is currently the most typical operational model in community embedded elderly care. Under the public construction and private operation model, the forms of public-private cooperation between the government, market, social organizations, and individuals are more diverse, and the threshold for service operation entities is relatively relaxed, making this operational model possess good practical operability and regional applicability.
In addition, the public construction and private operation model can maximize the activation of social elderly care service resources, promote quality services to sink to the grassroots, thereby better achieving the basic functional positioning of community embedded elderly care—allowing more elderly individuals to enjoy quality and inclusive elderly care services nearby.
In contrast, the private funding and assistance model is more distributed in regions with limited local financial capacity. Under this model, the construction funds for community embedded elderly care service facilities are primarily raised by private entities, while local governments only need to provide certain site and funding support. Therefore, this model helps further reduce the fiscal expenditure pressure on local governments. Market operation, collective economy, and charitable mutual assistance are three more niche operational models, with the market operation model primarily targeting elderly individuals with a certain economic foundation and a focus on quality of life, while the collective economy model is mainly found in regions with relatively developed village collective economies, and the charitable mutual assistance model is primarily distributed in rural and other underdeveloped areas.
Challenges Facing Community Embedded Elderly Care Practice
Despite the fact that some provincial and municipal regions have achieved certain results in community embedded elderly care, it remains in the exploratory stage. Community embedded elderly care in China still faces multiple challenges in practice, stemming from demand embedding, resource embedding, subject embedding, and concept embedding, which merits deeper reflection.
1. Demand Embedding: Mismatch in Supply and Demand Relationships, Lack of Effective Linking Mechanisms
On one hand, the supply and demand relationship of community embedded elderly care services exhibits a total imbalance. Influenced by traditional filial piety concepts, many elderly individuals are still unwilling to enter any facilities or places with social elderly care attributes or accept socialized elderly care services provided by non-family members. Furthermore, some elderly individuals have limited understanding of community embedded elderly care, leading them to adopt a cautious or rejecting attitude towards such elderly care service facilities, which also suppresses their related elderly care needs.
On the other hand, the supply and demand relationship of community embedded elderly care services exhibits structural imbalances, specifically reflected in two aspects: one is the mismatch between supply and demand in service projects. Research has found that many communities arrange different learning courses and cultural activities for elderly individuals every day, yet the actual effectiveness of these schedules is often unsatisfactory, with frequent occurrences of “overcrowded” and “unattended” extremes.
Clearly, this is due to the service providers’ inability to accurately grasp the needs of elderly individuals and their difficulty in flexibly adjusting service supply strategies. This superficial, rigid service supply model results in a waste of elderly care service resources. The second aspect is the mismatch in supply and demand among different regions, which is concentrated in the geographical spatial layout of community embedded elderly care service facilities not being coordinated with the scale and density of the elderly population within their regions.
Overall, the dual imbalance in the supply and demand relationship reveals the lack and inadequacy of demand linking mechanisms in the current development of community embedded elderly care. Although many regions have established digital elderly care information service platforms, research during the investigation found that most platforms are flashy but impractical, with missing basic data, outdated information updates, insufficient information accuracy, and system network delays, making it increasingly difficult for “services to find people.”
2. Resource Embedding: Limited Professional Service Personnel, Uneven Service Quality
Taking human resources as an example, the current elderly care service industry in China is labor-intensive. Due to practical factors such as high job pressure at the grassroots level, low salary levels, low social recognition, and limited development space, the development of community embedded elderly care is facing a severe personnel crisis, manifested in three aspects:
First, structural imbalance.The service workforce is aging, with a growing number of workers over the age of 50, and there are few young frontline personnel joining, resulting in a noticeable lack of development vitality. Additionally, the gender ratio of the service workforce is severely unbalanced, with a generally weak willingness among males to engage in related work.
Second, insufficient qualifications.There are widespread issues among workers regarding low educational levels and a lack of professional knowledge and skills. In some rural and underdeveloped regions, some workers can work directly without professional training or relevant qualifications, which may impact the quality of elderly care services and leave service risks.
Third, high turnover.During the research process, it was found that due to similar job attributes, many workers choose to switch to less stressful and more manageable domestic service jobs after working in institutions for a period of time. This leads to frequent recruitment and retraining of employees, and such high-frequency personnel turnover not only increases the cost of elderly care services but also negatively impacts service quality, hindering the long-term stable development of community embedded elderly care.
Besides frontline personnel, the development of community embedded elderly care also relies on specialized management. However, there are significant differences in the operational entities’ industry backgrounds, resource foundations, conceptual orientations, and professional levels, which may lead to substantial differences in the quality of community embedded elderly care services provided in various regions. The construction of evaluation systems and standardized management for related elderly care services remains a long-term and arduous task.
3. Subject Embedding: Interwoven Rights, Responsibilities, and Interests, Difficulty in Coordinating Multiple Subjects
Currently, the operational models of community embedded elderly care are rich and diverse, and the participating subjects in different models exhibit a diversified characteristic in practice. Therefore, in various links involving the interests and rights and responsibilities distribution of multiple subjects, it is inevitable that a series of coordination issues arise:
First, the construction of community embedded elderly care service facilities may, to some extent, encroach on the public land resources of the community. The renovation and subsequent operation of these facilities may also negatively impact community residents (noise pollution, influx of outsiders, etc.), which can provoke resistance and behaviors from residents, resulting in a neighborhood avoidance effect.
Second, in the construction and operation process of community embedded elderly care service facilities, private entities face strict qualification reviews, with fire safety reviews being particularly prominent. The complex review procedures, lengthy review cycles, and stringent review indicators significantly increase the costs and pressures of facility operations, which is unwelcoming for some grassroots operational entities.
Third, for public construction and private operation, private funding and assistance, and other public-private cooperation operational models, depending on different contract types, the management rights and operational rights, ownership, and usage rights of community embedded elderly care service facilities may appear to be separated to varying degrees, leading to deviations in action logic, competition between public and private entities, and biases in operational direction.
In addition, these issues also reflect the financial and land constraints faced in the development of community embedded elderly care, with the former concentrated on difficulties in timely and sufficient issuance of fiscal subsidies and limited risk resistance capabilities of small and micro institutions, while the latter is focused on limited available land resources in the community and difficulties in the approval of construction land for facilities.
4. Concept Embedding: Regional Foundations Exist Differently, Experience Paradigm Promotion is Blocked
The community embedded elderly care in China originated in Shanghai, a city with strong economic power and a high level of urbanization. Through long-term exploration and practice of this elderly care model, Shanghai has accumulated relatively rich experience. However, whether these experiences and paradigms are equally applicable to other regions is evidently a negative answer.
China’s vast territory features significant differences in natural geographical characteristics, economic development levels, basic population composition, and local cultural concepts among different regions, making it challenging to implement a standardized elderly care model nationwide. This is particularly reflected in:
First, the differences between developed and underdeveloped regions.Developing community embedded elderly care requires investment in land, labor, technology, and other resources, all of which ultimately rely on substantial financial support. The elderly care service industry has the unique attributes of high upfront investment and long return periods, making it difficult for economically underdeveloped regions with limited fiscal revenues to develop this elderly care model.
Second, the differences between urban and rural areas.Unlike urban areas, rural areas have relatively weak foundations for developing community embedded elderly care, and the available social resources for integration are extremely limited. Most rural communities require more support to develop this elderly care model. Furthermore, influenced by strong filial piety concepts, rural elderly individuals’ acceptance of social elderly care tends to be lower than that of urban elderly individuals.
Third, the differences between plain and mountainous areas.Compared to plain areas, mountainous regions have more complex terrain, more isolated transportation, and dispersed resident distribution. Communities here no longer conform to the “plain thinking” of community, and promoting community embedded elderly care in mountainous areas will face greater cost issues and a series of fairness issues in resource allocation.
Recommendations for Developing Community Embedded Elderly Care
In March 2023, Premier Li Qiang pointed out during a survey in Hainan that “home-based elderly care is the primary form of elderly care in our country. We must actively explore community embedded elderly care services around the needs and wishes of the elderly, addressing their needs for food and medical care.” In May of the same year, the Central Committee of the Communist Party of China and the State Council issued the “Opinions on Promoting the Construction of Basic Elderly Care Service Systems,” which listed the implementation of the national basic elderly care service list as a focus of national elderly care work in the near future.
The community, as the basic unit of residents’ lives and social governance, is the “last mile” for implementing the sinking of elderly care service resources to the grassroots and promoting the comprehensive implementation of basic elderly care services. This article believes that the important foundation for the development of elderly care services in China is community embedded elderly care, which involves both geographical space embedding and comprehensive embedding of real needs, facility resources, multiple subjects, and value concepts.Community embedded elderly care is not only a necessary path to achieve the goal of ensuring that all elderly individuals enjoy basic elderly care services but also a key direction and inevitable trend for the future development of modern elderly care models in China.
In this regard, governments, communities, enterprises, and social organizations should clarify their respective responsibilities, combine regional characteristics, rely on favorable resources, and work together to promote the high-quality development of community embedded elderly care. Specifically:
First, local governments should strive to change traditional governance concepts and methods, encouraging more market and social entities to participate in the supply of elderly care services. At the same time, they should clearly recognize their responsibilities in the development of elderly care services, as promoting community embedded elderly care cannot be separated from government policy support and guidance, and the operation of community embedded elderly care cannot be conducted without government coordination and supervision.
Second, grassroots communities should always fulfill their mission to serve residents, continuously improve the internal management and service system of the community, actively link various elderly care service resources based on the needs of elderly individuals in the community, and enhance the public service capacity of grassroots communities.
Finally, enterprises and social organizations should standardize service orientation and manage operations properly. The elderly care service industry itself has certain public welfare attributes; therefore, whether through public-private cooperation or market-oriented operations, operators should adhere to the principle of unifying economic and social benefits, aligning their efforts with the government’s original intention to develop community embedded elderly care.
So, what specific ways or means can we use to achieve the high-quality development goals of community embedded elderly care? Based on the multi-dimensional embedding issues mentioned above, the following four recommendations are proposed:
First, strengthen the construction of information platforms and optimize the service supply structure.Building and maintaining elderly care service information platforms is aimed at more timely, comprehensive, and accurate grasp of the real elderly care service needs of the elderly in the community. Therefore, it is essential to strengthen the construction of information platforms with a long-term vision and pragmatic attitude, ensuring that the “fundamentals” of hardware facilities, data collection, and information processing are well done, truly making the demand linking mechanism of elderly care services in the community practical, detailed, and sustainable. On this basis, service suppliers should also integrate social resources based on the actual elderly care service demand situation they grasp, timely adjust the relevant elderly care service projects to further optimize the supply structure of community embedded elderly care services.
Second, improve the working environment for frontline personnel and enhance the construction of the talent team.On one hand, while ensuring that the work content and intensity remain largely unchanged, gradually improve the salary and welfare levels of frontline personnel, paying attention to the physical and mental health of grassroots workers, and create a good and comfortable working environment to achieve the dual goals of reducing personnel turnover and stimulating employee enthusiasm. On the other hand, the government and social operators should gradually deepen cooperation with local vocational high schools, universities, and research institutes, actively exploring a talent integration mechanism from “talent training” to “talent delivery” through the establishment of professional internship sites, the construction of practical teaching bases, and the signing of targeted employment agreements to optimize the structure of the elderly care service talent team.
Third, consider the needs of multiple subjects and refine support policies.The sinking of quality elderly care service resources relies on the coordination of the government, support from the community, participation from society, and recognition from the masses. Therefore, in the development of community embedded elderly care, it is essential to fully listen to the demands of multiple subjects, balance the rights and interests of public and private sectors, and actively explore a cooperative mechanism of joint discussion, construction, and sharing, breaking down information barriers in the coordination process among multiple subjects to better eliminate institutional obstacles in the construction and operation of facilities and the supply of elderly care services. In addition, local governments should refine and implement relevant support policies for community embedded elderly care based on actual conditions, such as simplifying approval processes, providing tax incentives, expanding activity funding, and assisting in linking resources to ensure that government-related funds can be issued on time and in full.
Fourth, rely on local resource conditions and explore more embedding models.Community embedded elderly care does not have a fixed paradigm; blindly copying the development models of Shanghai, Beijing, and other places using “urban thinking” to develop rural areas or using “plain thinking” to examine mountainous areas will likely result in “mismatched conditions.” In fact, the primary focus of developing community embedded elderly care is to grasp the core, root in the local context, and adapt to local conditions. Local areas should fully utilize their advantageous resource conditions (such as land, funds, talent, markets, culture, etc.), emphasize the sinking and integration of resources, and explore development paths for embedded elderly care that align with local realities, such as rural communities in Datong City relying on collective economic self-construction of elder care homes, and the Charity Association of Yan’an County raising funds from multiple sources to build happy homes throughout the county.
(Text edited by: Tai Laojun Layout edited by: Tai Laoshi)
